Balke Selina, Weid Petra, Fangmann Laura, Rostin Paul, Henrich Wolfgang, Koenigbauer Josefine Theresia
Department of Obstetrics, Charité-Universitätsmedizin, 10117 Berlin, Germany.
J Clin Med. 2023 May 27;12(11):3709. doi: 10.3390/jcm12113709.
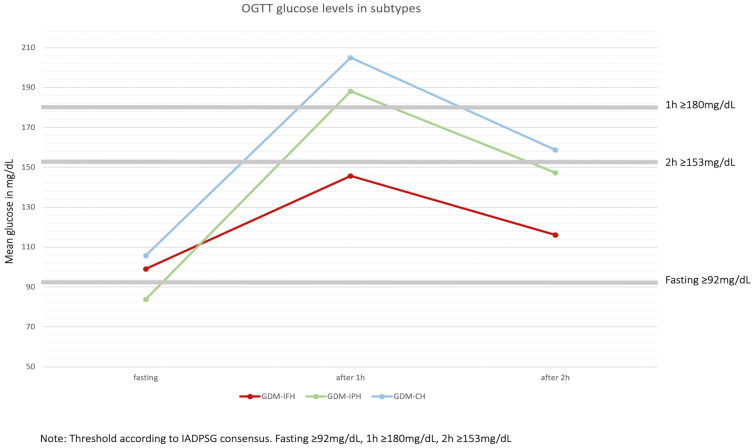
Gestational diabetes (GDM) is a common pregnancy complication defined as a glucose intolerance diagnosis during pregnancy. GDM is strongly associated with adverse fetal and maternal outcomes. In Germany, to screen and diagnose GDM we use a 1 h 50 g oGCT (oral glucose challenge test) followed by a 2 h 75 g oGTT if the first was pathological. This analysis examines the correlation of 75 g oGTT glucose levels and fetomaternal outcome.
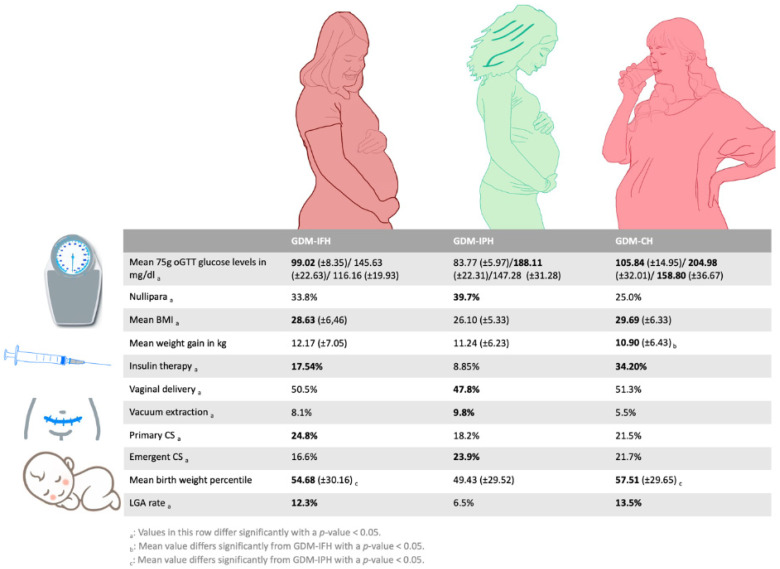
Data from 1664 patients from a gestational diabetes consultation clinic at the Charité University Hospital in Berlin, Germany, were analyzed retrospectively from 2015 to 2022. The 75 g oGTT blood glucose levels were categorized into isolated fasting hyperglycemia (GDM-IFH), isolated post-load hyperglycemia (GDM-IPH) and combined hyperglycemia (GDM-CH), using the levels of the fasting, 1 h and 2 h values, after glucose application. These subtypes were compared based on their baseline characteristics as well as fetal and maternal outcome.
GDM-IFH and GDM-CH women displayed higher pre-conceptional BMI and required insulin therapy more frequently ( < 0.001). The GDM-IFH group was at higher risk of having a primary cesarean section ( = 0.047), while GDM-IPH women were significantly more likely to have an emergent cesarean section ( = 0.013). The offspring of GDM-IFH and GDM-CH women were born with a significantly higher mean birthweight ( < 0.001) and birth weight percentiles ( < 0.001) and were at increased risk of being large for gestational age (LGA) ( = 0.004). Women from the GDM-IPH group delivered significantly more neonates who were small for gestational age ( = 0.027) or with low fetal weight <30th percentile ( = 0.003).
This analysis shows a strong association between the glucose response pattern in the 75 g oGTT and adverse perinatal fetomaternal outcome. The differences among the subgroups, specifically concerning insulin therapy, mode of delivery and fetal growth, suggest an individualized approach to prenatal care after a GDM diagnosis.
妊娠期糖尿病(GDM)是一种常见的妊娠并发症,定义为孕期诊断出的葡萄糖不耐受。GDM与不良的胎儿和母亲结局密切相关。在德国,为筛查和诊断GDM,我们采用1小时50克口服葡萄糖耐量试验(oGCT),如果首次试验结果异常,则接着进行2小时75克口服葡萄糖耐量试验(oGTT)。本分析旨在研究75克oGTT血糖水平与母婴结局之间的相关性。
对德国柏林夏里特大学医院妊娠期糖尿病咨询门诊2015年至2022年期间1664例患者的数据进行回顾性分析。根据葡萄糖服用后空腹、1小时和2小时的值,将75克oGTT血糖水平分为单纯空腹血糖升高(GDM - IFH)、单纯服糖后血糖升高(GDM - IPH)和联合血糖升高(GDM - CH)。比较这些亚组的基线特征以及胎儿和母亲结局。
GDM - IFH组和GDM - CH组女性孕前BMI较高,且更频繁地需要胰岛素治疗(<0.001)。GDM - IFH组进行初次剖宫产的风险较高(=0.047),而GDM - IPH组女性进行急诊剖宫产的可能性显著更高(=0.013)。GDM - IFH组和GDM - CH组女性的后代出生时平均出生体重显著更高(<0.001),出生体重百分位数也更高(<0.001),且大于胎龄(LGA)的风险增加(=0.004)。GDM - IPH组女性分娩的新生儿小于胎龄或胎儿体重低于第30百分位数的比例显著更高(=0.027)(=0.003)。
本分析表明75克oGTT中的葡萄糖反应模式与围产期母婴不良结局之间存在密切关联。亚组之间的差异,特别是在胰岛素治疗、分娩方式和胎儿生长方面,提示在GDM诊断后应采取个体化的产前护理方法。