Centre for Outcomes Research and Evaluation, McGill University Health Centre, Montreal, Quebec, Canada.
Division of Experimental Medicine, Department of Medicine, McGill University Health Centre, Montreal, Quebec, Canada.
JAMA Intern Med. 2024 Jan 1;184(1):18-27. doi: 10.1001/jamainternmed.2023.0699.
Despite widespread use, summary evidence from prior meta-analyses has contradictory conclusions regarding whether oseltamivir decreases the risk of hospitalization when given to outpatients. Several large investigator-initiated randomized clinical trials have not yet been meta-analyzed.
To assess the efficacy and safety of oseltamivir in preventing hospitalization among influenza-infected adult and adolescent outpatients.
PubMed, Ovid MEDLINE, Embase, Europe PubMed Central, Web of Science, Cochrane Central, ClinicalTrials.gov, and WHO International Clinical Trials Registry were searched from inception to January 4, 2022.
Included studies were randomized clinical trials comparing oseltamivir vs placebo or nonactive controls in outpatients with confirmed influenza infection.
In this systematic review and meta-analysis, Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) reporting guidelines were followed. Two independent reviewers (R.H. and É.B.C.) extracted data and assessed risk of bias using the Cochrane Risk of Bias Tool 2.0. Each effect size was pooled using a restricted maximum likelihood random effects model. The quality of evidence was graded using the Grading of Recommendations, Assessment, Development and Evaluations (GRADE) framework.
Hospitalization was pooled as risk ratio (RR) and risk difference (RD) estimates with 95% CIs.
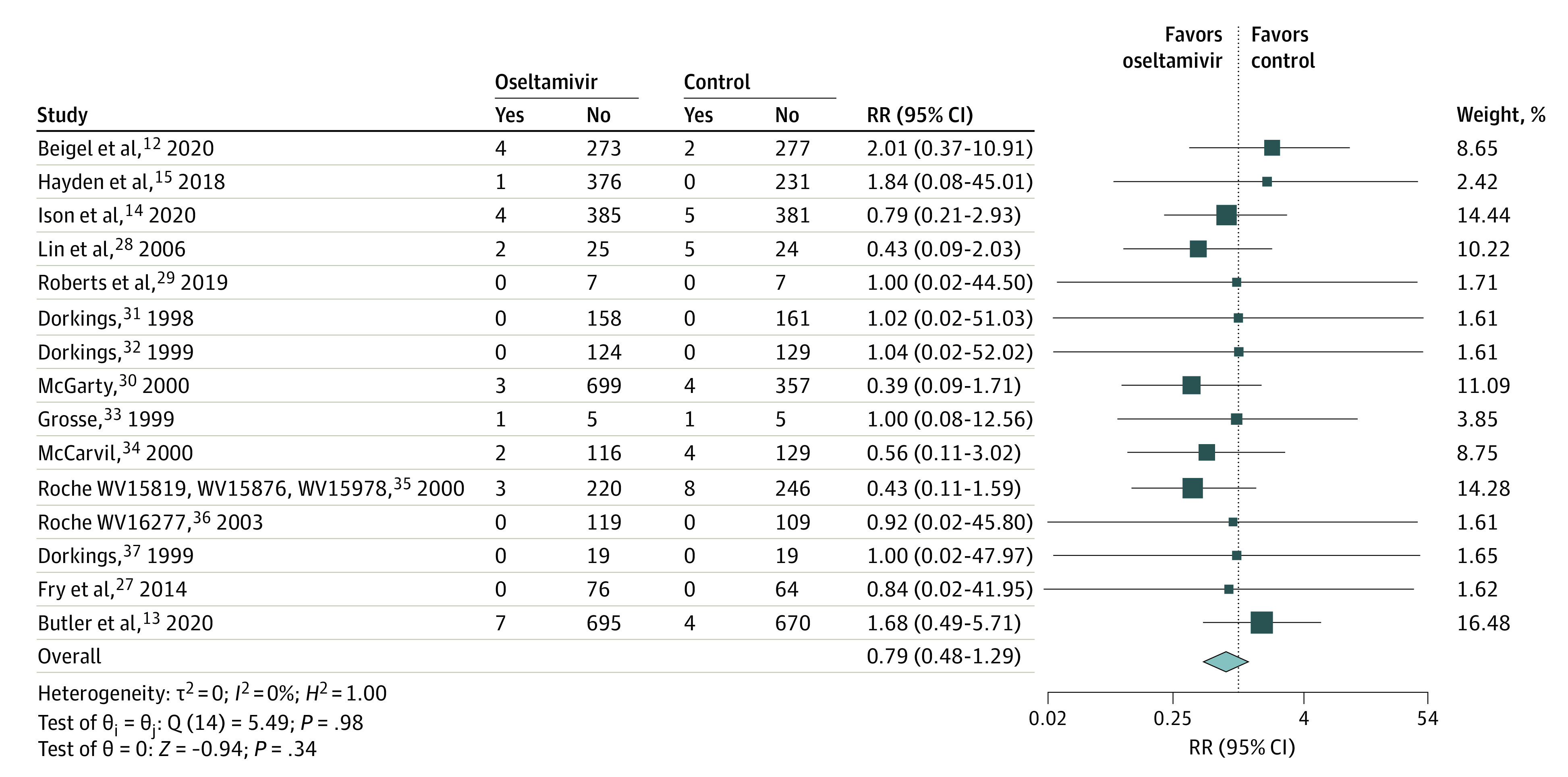
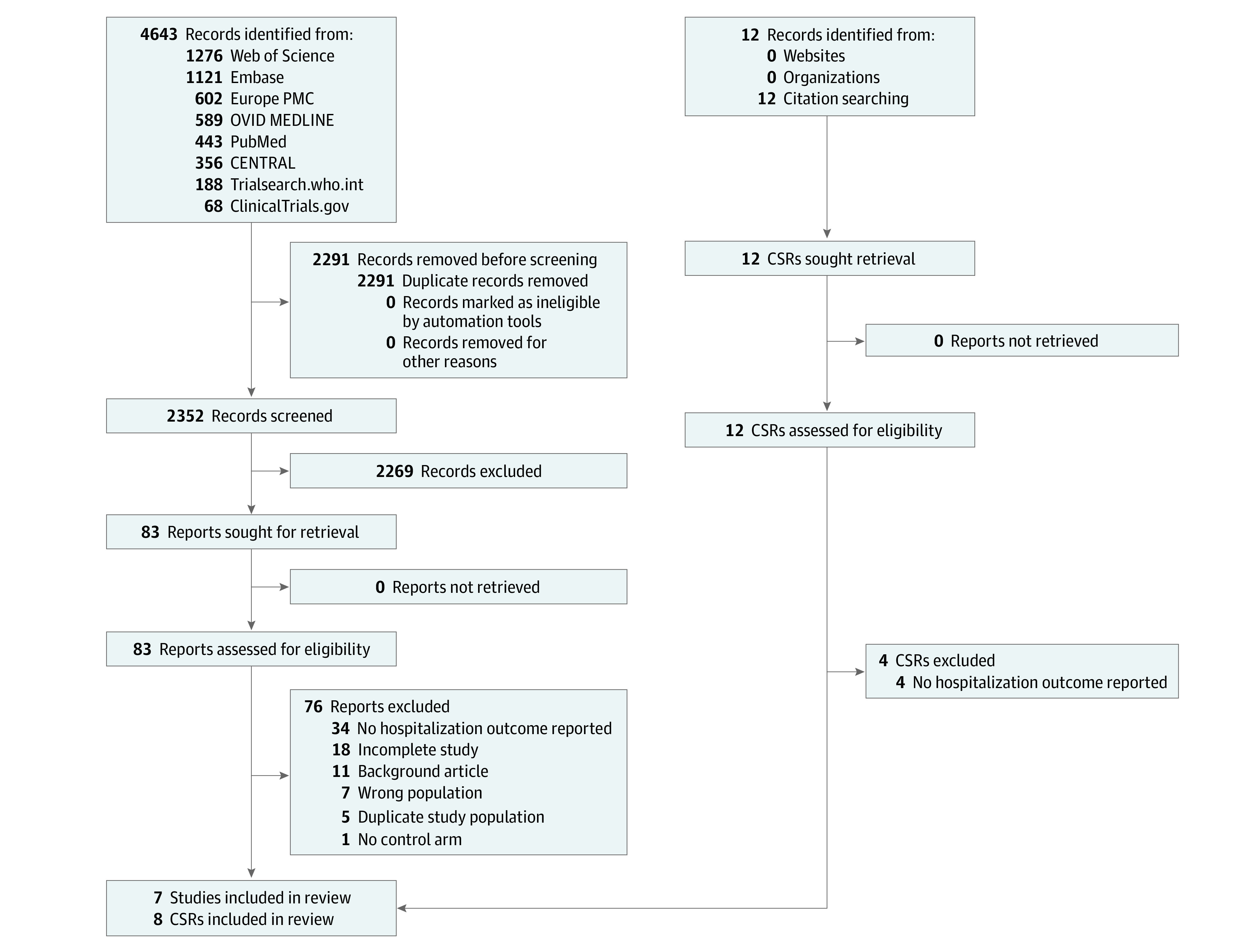
Of 2352 studies identified, 15 were included. The intention-to-treat infected (ITTi) population was comprised of 6166 individuals with 54.7% prescribed oseltamivir. Across study populations, 53.9% (5610 of 10 471) were female and the mean age was 45.3 (14.5) years. Overall, oseltamivir was not associated with reduced risk of hospitalization within the ITTi population (RR, 0.79; 95% CI, 0.48 to 1.29; RD, -0.17%; 95% CI, -0.23% to 0.48%). Oseltamivir was also not associated with reduced hospitalization in older populations (mean age ≥65 years: RR, 1.01; 95% CI, 0.21 to 4.90) or in patients considered at greater risk of hospitalization (RR, 0.65; 0.33 to 1.28). Within the safety population, oseltamivir was associated with increased nausea (RR, 1.43; 95% CI, 1.13 to 1.82) and vomiting (RR, 1.83; 95% CI, 1.28 to 2.63) but not serious adverse events (RR, 0.71; 95% CI, 0.46 to1.08).
In this systematic review and meta-analysis among influenza-infected outpatients, oseltamivir was not associated with a reduced risk of hospitalization but was associated with increased gastrointestinal adverse events. To justify continued use for this purpose, an adequately powered trial in a suitably high-risk population is justified.
尽管广泛使用,但先前荟萃分析的综合证据得出的结论相互矛盾,即奥司他韦是否能降低门诊流感感染患者的住院风险。一些大型的研究者发起的随机临床试验尚未进行荟萃分析。
评估奥司他韦在预防流感感染的成年和青少年门诊患者住院方面的疗效和安全性。
从建库到 2022 年 1 月 4 日,我们在 PubMed、Ovid MEDLINE、Embase、欧洲 PubMed 中心、Web of Science、Cochrane 中心、ClinicalTrials.gov 和世界卫生组织国际临床试验注册平台进行了检索。
纳入的研究是比较奥司他韦与安慰剂或非活性对照在确诊流感感染的门诊患者中的疗效和安全性的随机临床试验。
在这项系统评价和荟萃分析中,我们遵循了系统评价和荟萃分析的首选报告项目(PRISMA)报告准则。两位独立的审查员(R.H.和 É.B.C.)提取数据,并使用 Cochrane 偏倚风险工具 2.0 评估风险偏倚。使用限制性最大似然随机效应模型对每个效果大小进行汇总。使用推荐评估、制定与评价(GRADE)框架对证据质量进行分级。
住院率采用风险比(RR)和风险差(RD)估计值及其 95%置信区间(CI)表示。
在 2352 项研究中,有 15 项被纳入。意向治疗感染人群(ITTi)包括 6166 名接受奥司他韦治疗的流感感染患者,其中 54.7%的患者接受了奥司他韦治疗。在各研究人群中,53.9%(10471 名中的 5610 名)为女性,平均年龄为 45.3(14.5)岁。总体而言,奥司他韦并未降低 ITTi 人群的住院风险(RR,0.79;95%CI,0.48 至 1.29;RD,-0.17%;95%CI,-0.23%至 0.48%)。奥司他韦也不能降低老年人群(平均年龄≥65 岁:RR,1.01;95%CI,0.21 至 4.90)或被认为更易住院的患者的住院率(RR,0.65;95%CI,0.33 至 1.28)。在安全性人群中,奥司他韦与恶心(RR,1.43;95%CI,1.13 至 1.82)和呕吐(RR,1.83;95%CI,1.28 至 2.63)的发生率增加有关,但与严重不良事件(RR,0.71;95%CI,0.46 至 1.08)无关。
在这项针对流感感染门诊患者的系统评价和荟萃分析中,奥司他韦与降低住院风险无关,但与胃肠道不良事件的发生率增加有关。为了证明继续以此为目的使用奥司他韦是合理的,有必要在适当高风险人群中进行一项足够大的试验。