Faculdade de Medicina, Universidade Federal de Mato Grosso do Sul, Av. Senador Filinto Muller, s/n Cidade Universitária, Campo Grande, MS, 79070-900, Brazil.
Hospital Universitário Maria Aparecida Pedrossian, Universidade Federal de Mato Grosso do Sul, Campo Grande, MS, 79070-900, Brazil.
J Med Case Rep. 2023 Jun 13;17(1):241. doi: 10.1186/s13256-023-03963-5.
Insulinomas are rare neuroendocrine tumors that typically present with hypoglycemic crises. Peripheral neuropathy is an uncommon complication of insulinoma. Most clinicians expect peripheral neuropathy symptoms to reverse completely after the insulin-secreting tumor is resected, but this may be a misassumption.
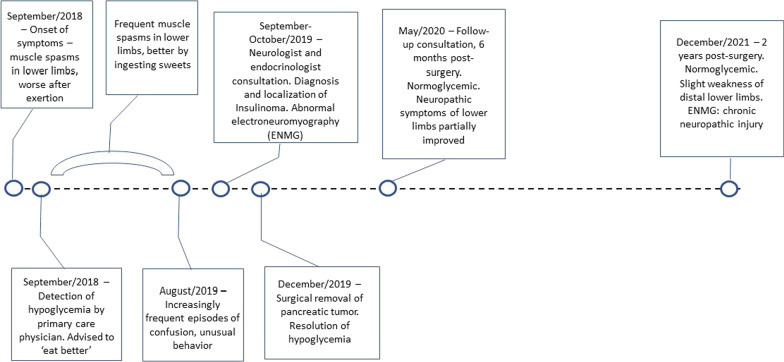
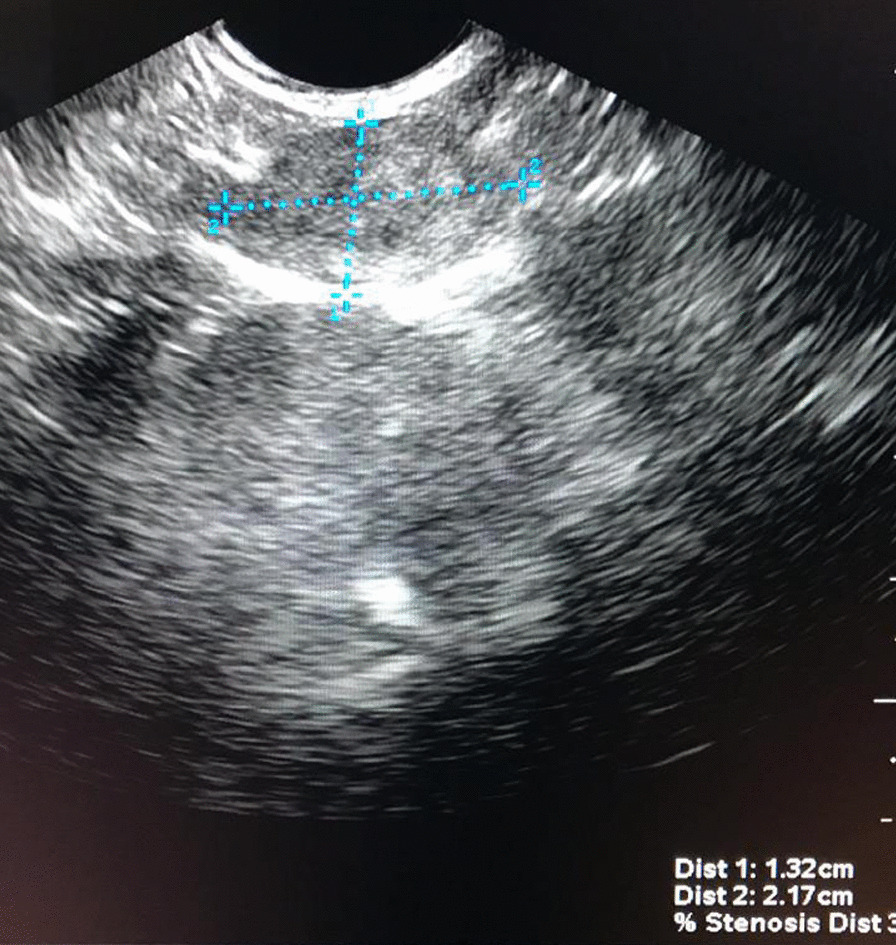
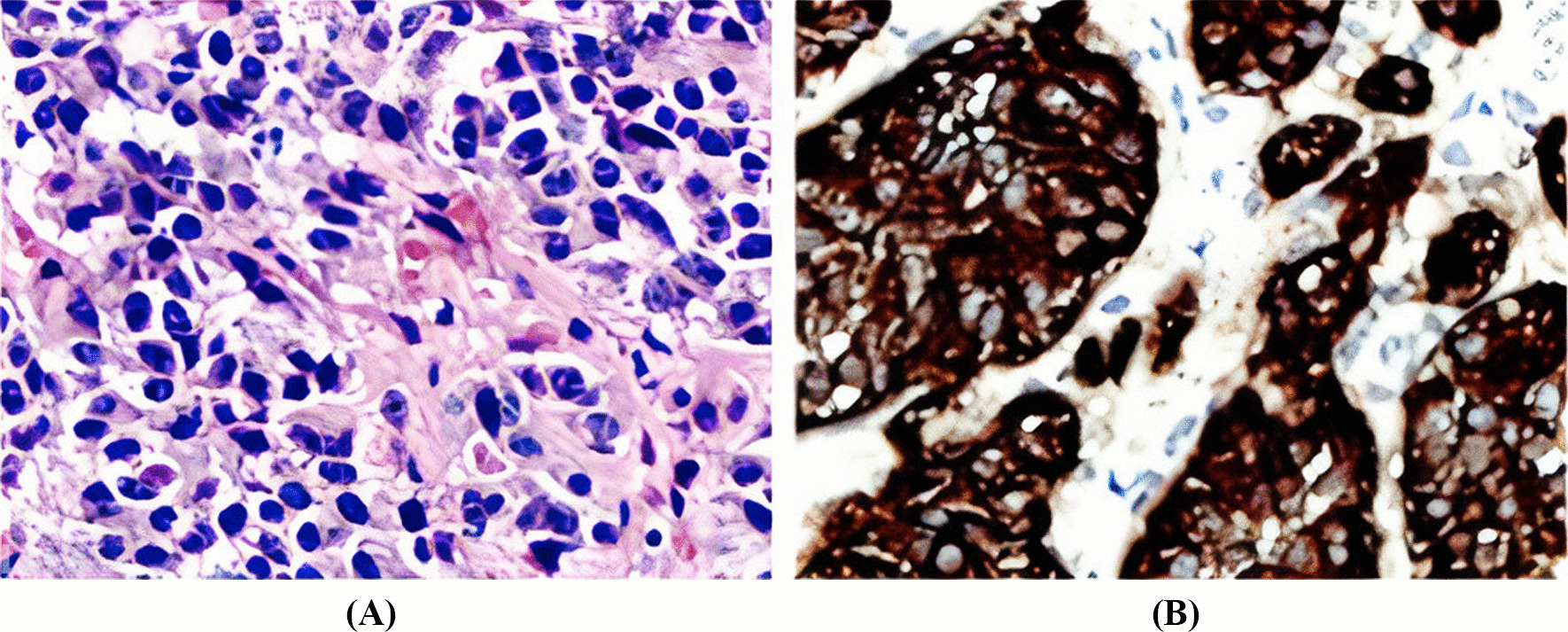
We report a case of a 16-year-old Brazilian boy with clonic muscle spasms of the lower limbs for almost one year. Disabling paraparesis and confusional episodes had progressively set in as well. There were no sensorial abnormalities in the lower limbs, upper limbs or cranial nerves. An electromyography revealed a motor neuropathy of the lower limbs. The diagnosis of insulinoma was established as serum insulin and C-peptide concentrations were inappropriately normal during spontaneous episodes of hypoglycemia. Following a normal abdominal magnetic resonance scan, the imaging work-up continued with an endoscopic ultrasound, which localized the tumor at the pancreatic body-tail transition. Once localized, a prompt surgical removal (enucleation) of the tumor was undertaken, leading to an immediate and complete resolution of hypoglycemia. The time length between the onset of symptoms and tumor resection was 15 months. After surgery, the symptoms of peripheral neuropathy of the lower limbs showed a slow and only partial improvement. At a two-year follow-up after surgery, although being able to lead a normal and productive life, the patient still reported symptoms of reduced muscular strength in the lower limbs and a new electroneuromyography analysis showed chronic denervation and reinnervation in the legs' muscles-indicating chronic neuropathic injury.
The events of this case reinforce the importance of an agile diagnostic work-up and spry definitive treatment for patients with this uncommon disease, enabling the cure of neuroglycopenia before permanent bothersome complications ensue.
胰岛素瘤是一种罕见的神经内分泌肿瘤,通常表现为低血糖危象。周围神经病变是胰岛素瘤的一种罕见并发症。大多数临床医生认为,在切除胰岛素分泌肿瘤后,周围神经病变症状会完全逆转,但这可能是一种误解。
我们报告了一例 16 岁巴西男孩,下肢出现痉挛性肌肉抽搐近一年。下肢无力和意识混乱逐渐加重。下肢、上肢或颅神经无感觉异常。肌电图显示下肢运动神经病。在自发性低血糖发作期间,血清胰岛素和 C 肽浓度不适当正常,诊断为胰岛素瘤。腹部磁共振扫描正常后,影像学检查继续进行内镜超声检查,将肿瘤定位在胰体-胰尾交界处。一旦定位,迅速进行肿瘤切除术(剜除术),导致低血糖立即完全缓解。症状出现与肿瘤切除之间的时间长度为 15 个月。手术后,下肢周围神经病的症状缓慢且仅部分改善。手术后两年随访时,尽管患者能够过上正常和富有成效的生活,但仍报告下肢肌肉力量减弱,新的肌电图分析显示腿部肌肉存在慢性去神经和再神经支配,表明存在慢性神经损伤。
该病例的发生事件强调了对这种罕见疾病进行敏捷诊断和快速确定性治疗的重要性,以便在永久性麻烦的并发症发生之前治愈神经低血糖症。