Department of Health Law, Policy, and Management, School of Public Health, Boston University, Boston, MA, USA.
Vanderbilt University Medical Center, Nashville, TN, USA.
Inquiry. 2023 Jan-Dec;60:469580231182512. doi: 10.1177/00469580231182512.
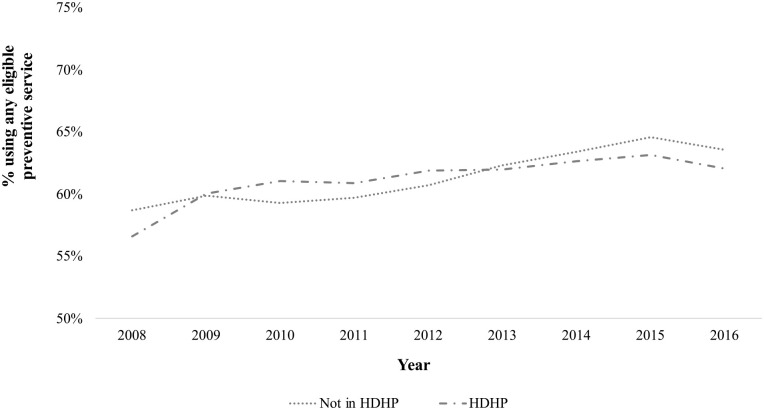
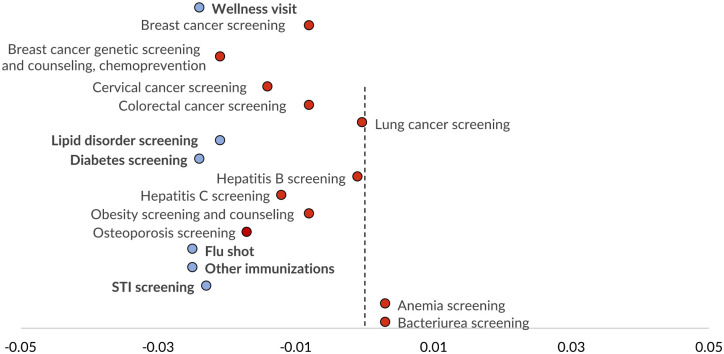
The Affordable Care Act aimed to increase use of preventive services by eliminating cost-sharing to consumers. However, patients may be unaware of this benefit or they may not seek preventive services if they anticipate that the cost of potential diagnostic or treatment services will be too high, both more likely among those in high deductible health plans. We used nationally representative private health insurance claims (100% sample of IBM MarketScan) for the United States from 2006 to 2018, restricting the data to enrollment and claims for non-elderly adults who were enrolled for the full plan year. The cross-sectional sample (185 million person-years) is used to describe trends in preventive service use and costs from 2008 through 2016. The cohort sample (9 million people) focuses on the elimination of cost-sharing for certain high-value preventive services in late 2010, requiring continuous enrollment across 2010 and 2011. We examine whether HDHP enrollment is associated with use of eligible preventive services using semi-parametric difference-in-differences to account for endogenous plan selection. Our preferred model implies that HDHP enrollment was associated with a reduction of the post-ACA change in any use of eligible preventive services by 0.2 percentage points or 12.5%. Cancer screenings were unaffected but HDHP enrollment was associated with smaller increases in wellness visits, immunizations, and screening for chronic conditions and sexually transmitted infections. We also find that the policy was ineffective at reducing out-of-pocket costs for the eligible preventive services, likely due to implementation issues.
平价医疗法案旨在通过取消消费者的自付费用来增加预防性服务的使用。然而,如果患者预期潜在诊断或治疗服务的费用过高,他们可能不知道这一好处,或者他们可能不会寻求预防性服务,这种情况在高免赔额健康计划中更为常见。我们使用了 2006 年至 2018 年美国具有代表性的私人健康保险索赔数据(IBM MarketScan 的 100%样本),将数据限制在非老年成年人的整个计划年度的登记和索赔范围内。横截面样本(1.85 亿人年)用于描述 2008 年至 2016 年期间预防性服务使用和费用的趋势。队列样本(900 万人)侧重于 2010 年末消除某些高价值预防性服务的自付费用,需要在 2010 年和 2011 年连续登记。我们使用半参数差分差异来检查高免赔额健康计划的登记是否与合格预防性服务的使用相关,以解释内生计划选择。我们首选的模型表明,高免赔额健康计划的登记与合格预防性服务的任何使用的 ACA 后变化减少 0.2 个百分点或 12.5%相关。癌症筛查不受影响,但高免赔额健康计划的登记与健康检查、免疫接种以及慢性疾病和性传播感染的筛查的增加幅度较小有关。我们还发现,该政策在降低合格预防性服务的自付费用方面效果不佳,可能是由于实施问题。