Department of Obstetrics and Gynecology, Division of Female Pelvic Medicine and Reconstructive Surgery, Eastern Virginia Medical School, 825 Fairfax Avenue, Suite 526, Norfolk, VG, 23507-2007, USA.
Faculty of Medicine, Department of Obstetrics and Gynecology, University of Debrecen, Pf 400, Debrecen, 4002, Hungary.
BMC Womens Health. 2023 Jun 20;23(1):321. doi: 10.1186/s12905-023-02476-z.
Pelvic floor muscle training (PFMT) is the first-line treatment approach for stress urinary incontinence. Creatine and leucine have been shown to improve muscle function. Our aim was to assess the effectiveness of a food supplement and PFMT in women with stress-predominant urinary incontinence.
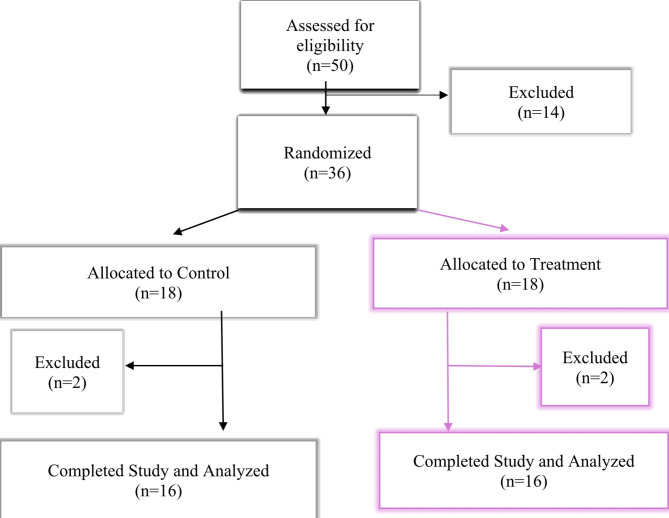
Women with stress-predominant urinary incontinence were randomized in 1:1 ratio to receive daily oral supplementation for six weeks with either a food supplement (treatment group) or placebo (control group). Both groups were instructed to perform standardized daily PFMT. The primary outcome was the Urogenital Distress Inventory Short Form (UDI-6) score. Secondary outcomes were the Incontinence Impact Questionnaire (IIQ-7) score, Patient's Global Impression of Severity (PGI-S), and Biomechanical Integrity score (BI-score) measured by Vaginal Tactile Imager. To have a power of 80% and a significance level of 5% to detect a decrease of 16 points in the UDI-6 score, a sample size of 32 was needed, with 16 patients in each arm of our trial.
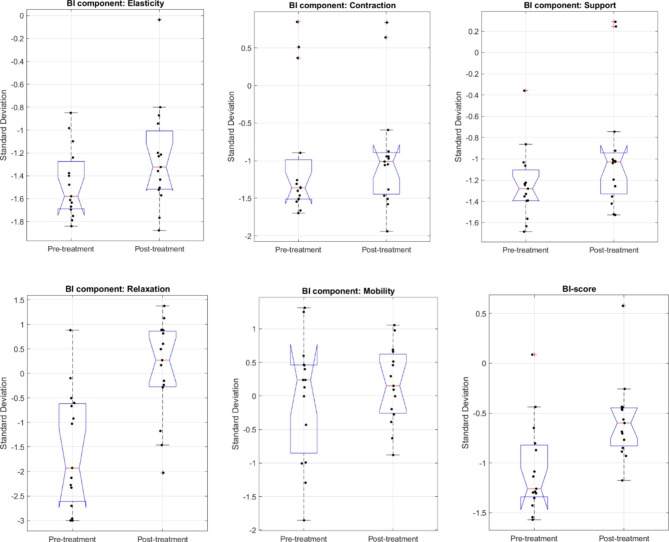
Sixteen women in the control group and sixteen in the treatment group completed the trial. Between-group analysis revealed no significant differences between the control and treatment group except for mean change (delta) in vaginal squeeze pressure [(cmH2O, mean ± SD), 5 ± 12 vs. 15 ± 15, P = 0.04] and mean change (delta) in PGI-S score [(mean ± SD), -0.2 ± 0.9 vs. -0.8 ± 0.8, P = 0.04]. Within-group analysis showed that UDI-6 and IIQ-7 scores improved significantly from baseline to six weeks in the treatment group but not in the control group [UDI-6 score (mean ± SD) 45 ± 21 vs. 29 ± 21, P = 0.02; 43 ± 18 vs. 33 ± 26, P = 0.22] [IIQ-7 score (mean ± SD) 50 ± 30 vs. 30 ± 21, P = 0.01; 48 ± 23 vs.40 ± 28, P = 0.36]. PGI-S scores only improved in the treatment group from baseline to six weeks after treatment [PGI-S score (mean ± SD) 3.1 ± 0.8 vs. 2.3 ± 0.8, P = 0.0001]. BI-score, on average, improved significantly in the treatment and control group as well [SD unit, mean, from - 1.06 to -0.58, P = 0.001; from - 0.66 to -0.42, P = 0.04].
Women with stress-predominant urinary incontinence receiving a specially formulated supplement in addition to daily PFMT for six weeks had significantly improved urinary symptoms (decrease in UDI-6 score and IIQ-7) and BI-score compared to their baseline.
ClinicalTrials.gov Identifier: NCT05358769. 27/04/2022.
盆底肌训练(PFMT)是治疗压力性尿失禁的首选方法。已经证明肌酸和亮氨酸可以改善肌肉功能。我们的目的是评估一种饮食补充剂和 PFMT 在以压力为主的尿失禁女性中的疗效。
将以压力为主的尿失禁女性随机分为 1:1 比例,每天口服补充剂 6 周,一组接受饮食补充剂(治疗组),另一组接受安慰剂(对照组)。两组均接受标准化每日 PFMT。主要结局是尿失禁生活质量问卷短表(UDI-6)评分。次要结局是尿失禁影响问卷(IIQ-7)评分、患者总体严重程度评分(PGI-S)和阴道触觉成像测量的生物力学完整性评分(BI-score)。为了有 80%的功效和 5%的显著性水平来检测 UDI-6 评分降低 16 分,我们的试验需要 32 名患者,每组 16 名。
对照组和治疗组各有 16 名女性完成了试验。组间分析显示,除阴道挤压压力的平均变化(cmH2O,均值±标准差)[5±12 比 15±15,P=0.04]和 PGI-S 评分的平均变化(均值±标准差)[-0.2±0.9 比-0.8±0.8,P=0.04]外,对照组和治疗组之间无显著差异。组内分析显示,治疗组 UDI-6 和 IIQ-7 评分从基线到 6 周时显著改善,但对照组无改善[UDI-6 评分(均值±标准差)45±21 比 29±21,P=0.02;43±18 比 33±26,P=0.22] [IIQ-7 评分(均值±标准差)50±30 比 30±21,P=0.01;48±23 比 40±28,P=0.36]。PGI-S 评分仅在治疗组中从基线到治疗 6 周后改善[PGI-S 评分(均值±标准差)3.1±0.8 比 2.3±0.8,P=0.0001]。BI 评分在治疗组和对照组中也有显著改善[SD 单位,均值,从-1.06 到-0.58,P=0.001;从-0.66 到-0.42,P=0.04]。
与基线相比,接受专门配方补充剂加每日 PFMT 治疗 6 周的以压力为主的尿失禁女性,其尿失禁症状(UDI-6 评分和 IIQ-7 降低)和 BI 评分显著改善。
ClinicalTrials.gov 标识符:NCT05358769. 27/04/2022。