Senguttuvan Nagendra Boopathy, Bhatt Hemal, Balakrishnan Vinod Kumar, Krishnamoorthy Parasuram, Goel Sunny, Reddy Pothireddy M K, Subramanian Vinodhini, Claessen Bimmer E, Kumar Ashish, Majmundar Monil, Ro Richard, Lerakis Stamatios, Jayaraj Ramamoorthi, Kalra Ankur, Flather Marcus, Dangas George, Tang Gilbert H L
Department of Cardiology, Sri Ramachandra Institute of Higher Education and Research, Chennai, India.
Department of Cardiology, The Zena and Michael A. Wiener Cardiovascular Institute, Icahn School of Medicine at Mount Sinai, New York, NY, United States.
Front Cardiovasc Med. 2023 May 25;10:1130354. doi: 10.3389/fcvm.2023.1130354. eCollection 2023.
Transfemoral Trans-catheter Aortic Valve Replacement (TF-TAVR) is a safe and effective therapy compared with surgical aortic valve replacement (SAVR) in patients across all risk profiles using balloon-expandable valves (BEV) and self-expanding valves (SEV). Our aim was to compare safety and efficacy of BEV vs. SEV in high-risk patients undergoing TF-TAVR.
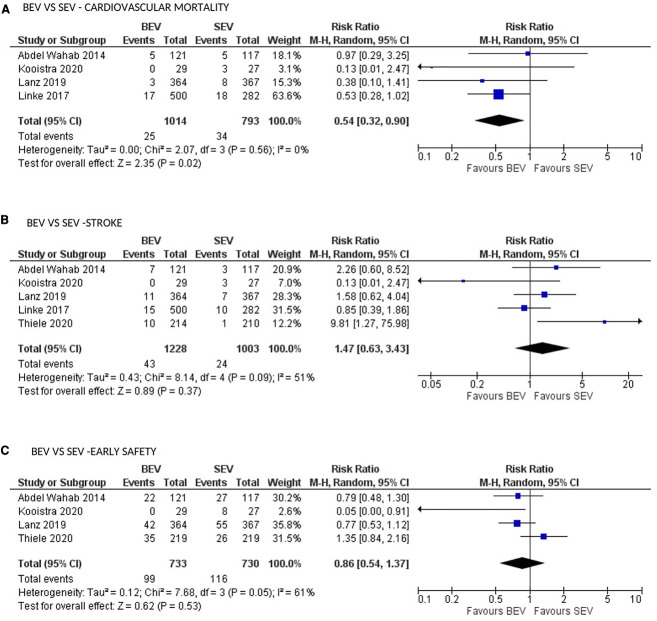
We searched PubMed, EMBASE, Clinicaltrials.gov, Scopus, and Web of sciences for studies on patients with severe aortic stenosis undergoing TAVR. Primary outcome was 30-day all-cause mortality. Secondary outcomes defined by Valve Academic Research Consortium 2 (VARC-2) criteria were also examined. Six studies with 2,935 patients (1,439 to BEV and 1,496 to SEV) were included. BEV was associated with lower risk of all-cause mortality (2.2% vs. 4.5%; RR: 0.51; 95% CI: 0.31-0.82; < 0.006) and cardiovascular mortality [(2.5% vs. 4.3%; RR: 0.54; 95% CI: 0.32-0.90; = 0.01) at 30 days compared with SEV. Implantation of more than one valve per procedure (0.78% vs. 5.11%; RR: 0.15; 95% CI: 0.07-0.31; < 0.00001), and moderate/severe AR/PVL (2.5% vs. 9.01%; RR: 0.3; 95% CI: 0.17-0.48); < 0.00001) were also lower in the BEV arm.
BEV TAVR is associated with reduced all-cause mortality (High level of GRADE evidence), cardiovascular mortality (very low level) at 30 days compared with SEV TAVR in high surgical risk patients. Data are necessary to determine if the difference in outcomes persists in longer-term and if the same effects are seen in lower-risk patients.
identifier, CRD42020181190.
对于使用球囊扩张瓣膜(BEV)和自膨胀瓣膜(SEV)的所有风险状况的患者,经股动脉经导管主动脉瓣置换术(TF-TAVR)与外科主动脉瓣置换术(SAVR)相比是一种安全有效的治疗方法。我们的目的是比较在接受TF-TAVR的高危患者中BEV与SEV的安全性和有效性。
我们在PubMed、EMBASE、Clinicaltrials.gov、Scopus和Web of sciences中搜索了关于接受TAVR的严重主动脉瓣狭窄患者的研究。主要结局是30天全因死亡率。还检查了根据瓣膜学术研究联盟2(VARC-2)标准定义的次要结局。纳入了6项研究,共2935例患者(1439例接受BEV,1496例接受SEV)。与SEV相比,BEV在30天时全因死亡率风险较低(2.2%对4.5%;RR:0.51;95%CI:0.31-0.82;P<0.006),心血管死亡率也较低(2.5%对4.3%;RR:0.54;95%CI:0.32-0.90;P=0.01)。每次手术植入一个以上瓣膜的情况较少(0.78%对5.11%;RR:0.15;95%CI:0.07-0.31;P<0.00001),中度/重度主动脉瓣反流/瓣周漏的情况也较少(2.5%对9.01%;RR:0.3;95%CI:0.17-0.48;P<0.00001),均在BEV组中更低。
在高手术风险患者中,与SEV TAVR相比,BEV TAVR在30天时全因死亡率降低(证据等级高),心血管死亡率降低(证据等级非常低)。需要数据来确定结局差异在长期是否持续存在以及在低风险患者中是否也有相同的效果。
标识符,CRD42020181190。