School of Public Heath, University of Illinois at Chicago, Chicago, IL, USA.
Center of Innovation for Complex Chronic Healthcare, Hines VA Hospital, Hines, IL, USA.
BMC Infect Dis. 2023 Jun 23;23(1):427. doi: 10.1186/s12879-023-08400-y.
No research has been conducted to assess whether antibiotic prophylaxis prescribing differs by dental setting. Therefore, the goal of this study was to compare the prescribing of antibiotic prophylaxis in Veterans Affairs (VA) and non-Veterans Affairs settings.
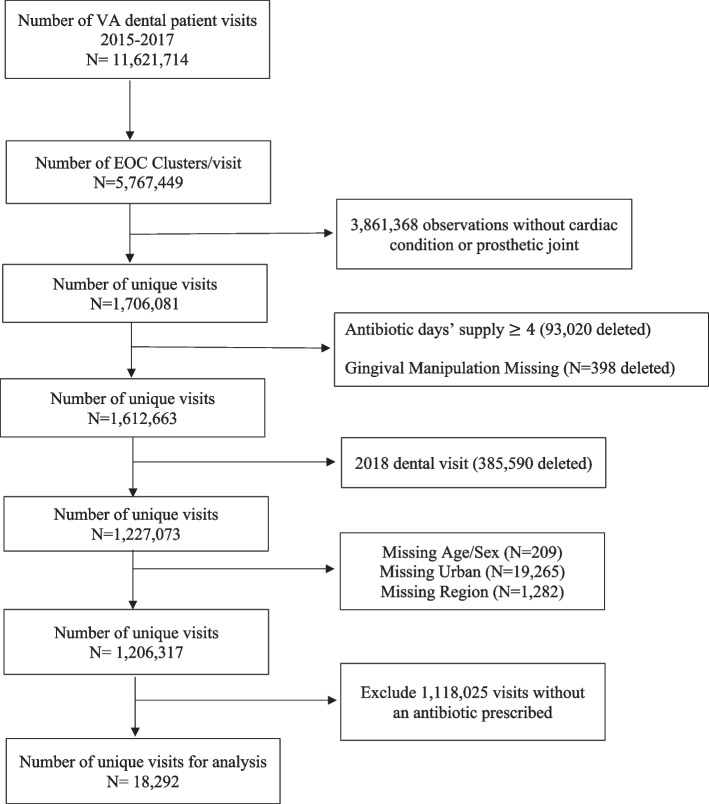
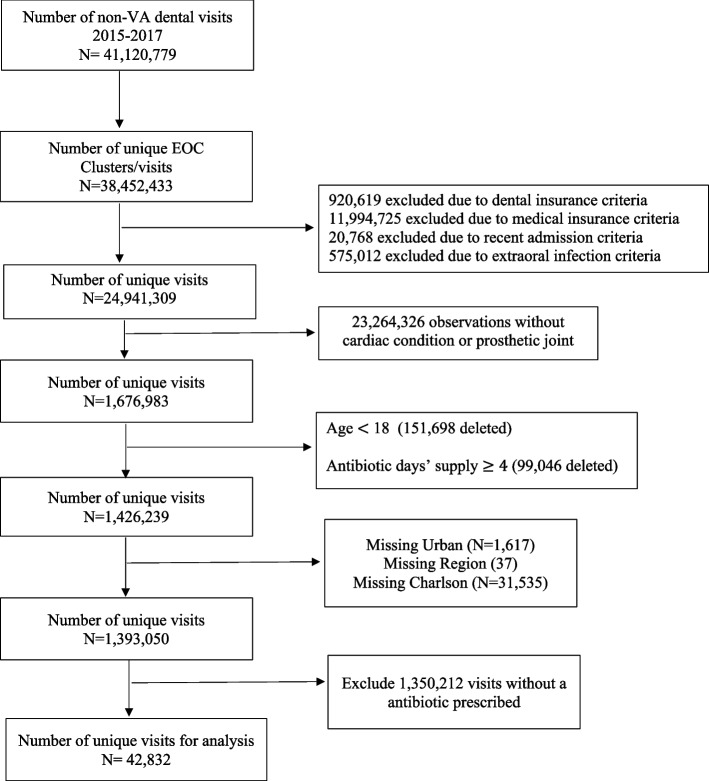
This was a retrospective study of veteran and non-veteran dental patients with cardiac conditions or prosthetic joints between 2015-2017. Multivariable log binomial regression analysis was conducted to compare concordant prescribing by setting with a sub-analysis for errors of dosing based on antibiotic duration (i.e., days prescribed).
A total of 61,124 dental visits that received a prophylactic antibiotic were included. Most were male (61.0%), and 55 years of age or older (76.2%). Nearly a third (32.7%) received guideline concordant prophylaxis. VA dental settings had a lower prevalence of guideline concordant prescribing compared to non-VA settings in unadjusted results (unadjusted prevalence ratio [uPR] = 0.92, 95% CI: 0.90-0.95). After adjustment, prevalence of guideline concordant prescribing was higher in those with prosthetic joints in the VA setting (adjusted prevalence ratio [aPR] = 1.73, 95% CI: 1.59-1.88), with no difference identified in those without a prosthetic joint (aPR = 0.99, 95% CI: 0.96-1.01). Concordance of dosing was higher in VA compared to non-VA settings (aPR = 1.11, 95% CI: 1.07-1.15).
VA has a higher prevalence of guideline concordant prescribing among those with prosthetic joints and when assessing dosing errors. Though the presence of an integrated electronic health record (EHR) may be contributing to these differences, other system or prescriber-related factors may be responsible. Future studies should focus on to what extent the integrated EHR may be responsible for increased guideline concordant prescribing in the VA setting.
目前尚未有研究评估口腔诊疗环境是否会影响抗生素预防用药的开具。因此,本研究旨在比较退伍军人事务部(VA)和非退伍军人事务部口腔诊疗环境下预防用抗生素的开具情况。
这是一项针对 2015 年至 2017 年间患有心脏疾病或人工关节的退伍军人和非退伍军人牙科患者的回顾性研究。采用多变量二项式回归分析比较不同口腔诊疗环境下的一致性用药,并对基于抗生素持续时间(即开具的天数)的剂量错误进行亚分析。
共纳入 61124 例接受预防性抗生素治疗的牙科就诊。大多数患者为男性(61.0%),年龄在 55 岁及以上(76.2%)。近三分之一(32.7%)的患者接受了指南一致的预防用药。未经调整的结果显示,VA 口腔诊疗环境下,与非 VA 环境相比,指南一致的预防用药的比例较低(未经调整的患病率比[uPR]=0.92,95%可信区间:0.90-0.95)。调整后,在 VA 环境下有假体关节的患者中,指南一致的预防用药比例更高(调整后的患病率比[aPR]=1.73,95%可信区间:1.59-1.88),而无假体关节的患者中未发现差异(aPR=0.99,95%可信区间:0.96-1.01)。VA 口腔诊疗环境下的剂量一致性比非 VA 环境更高(aPR=1.11,95%可信区间:1.07-1.15)。
VA 环境中在有假体关节的患者和评估剂量错误时,更倾向于遵循指南开具预防用抗生素。尽管存在集成电子健康记录(EHR)可能是造成这些差异的原因之一,但其他系统或处方相关因素也可能是造成差异的原因。未来的研究应侧重于评估集成 EHR 可能在多大程度上导致 VA 环境下更符合指南的预防用抗生素的开具。