Department of Epidemiology and Center for AIDS and STD, University of Washington, Seattle, Washington, USA.
Department of Epidemiology, University of Washington, Seattle, Washington, USA.
Clin Infect Dis. 2023 Nov 17;77(10):1449-1459. doi: 10.1093/cid/ciad405.
Mycoplasma genitalium (MG) is on the CDC Watch List of Antimicrobial Resistance Threats, yet there is no systematic surveillance to monitor change.
We initiated surveillance in sexual health clinics in 6 cities, selecting a quota sample of urogenital specimens tested for gonorrhea and/or chlamydia. We abstracted patient data from medical records and detected MG and macrolide-resistance mutations (MRMs) by nucleic acid amplification testing. We used Poisson regression to estimate adjusted prevalence ratios (aPRs) and 95% CIs, adjusting for sampling criteria (site, birth sex, symptom status).
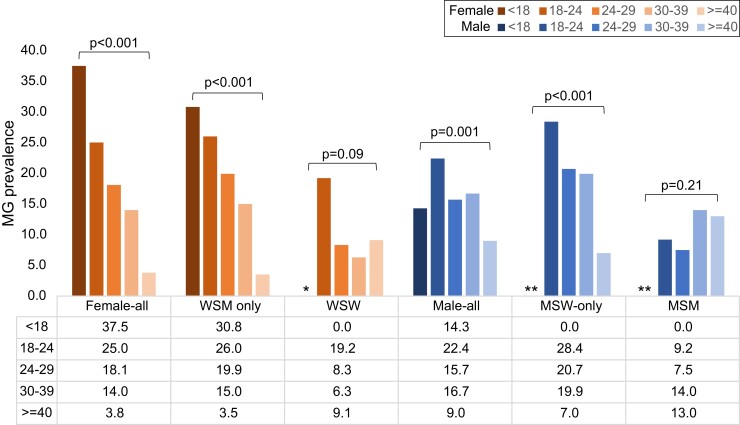
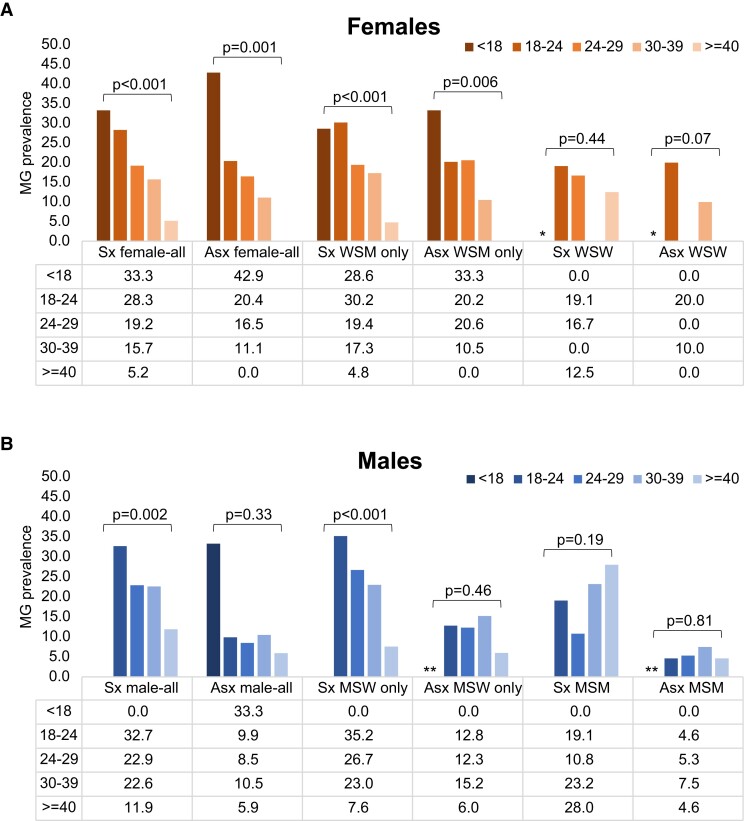
From October-December 2020 we tested 1743 urogenital specimens: 57.0% from males, 46.1% from non-Hispanic Black persons, and 43.8% from symptomatic patients. MG prevalence was 16.6% (95% CI: 14.9-18.5%; site-specific range: 9.9-23.5%) and higher in St Louis (aPR: 1.9; 1.27-2.85), Greensboro (aPR: 1.8; 1.18-2.79), and Denver (aPR: 1.7; 1.12-2.44) than Seattle. Prevalence was highest in persons <18 years (30.4%) and declined 3% per each additional year of age (aPR: .97; .955-.982). MG was detected in 26.8%, 21.1%, 11.8%, and 15.4% of urethritis, vaginitis, cervicitis, and pelvic inflammatory disease (PID), respectively. It was present in 9% of asymptomatic males and 15.4% of asymptomatic females, and associated with male urethritis (aPR: 1.7; 1.22-2.50) and chlamydia (aPR: 1.7; 1.13-2.53). MRM prevalence was 59.1% (95% CI: 53.1-64.8%; site-specific range: 51.3-70.6%). MRMs were associated with vaginitis (aPR: 1.8; 1.14-2.85), cervicitis (aPR: 3.5; 1.69-7.30), and PID cervicitis (aPR: 1.8; 1.09-3.08).
MG infection is common in persons at high risk of sexually transmitted infections; testing symptomatic patients would facilitate appropriate therapy. Macrolide resistance is high and azithromycin should not be used without resistance testing.
支原体生殖器(MG)是疾病预防控制中心(CDC)对抗菌药物耐药性威胁的监测清单上的一种病原体,然而目前还没有系统的监测来监测其变化。
我们在 6 个城市的性健康诊所启动了监测,选择淋病和/或衣原体检测的尿生殖标本进行定量抽样。我们从病历中提取患者数据,并通过核酸扩增检测检测 MG 和大环内酯类药物耐药性突变(MRM)。我们使用泊松回归来估计调整后的患病率比值(aPR)和 95%置信区间(CI),并根据采样标准(地点、出生性别、症状状态)进行调整。
2020 年 10 月至 12 月,我们检测了 1743 份尿生殖标本:57.0%来自男性,46.1%来自非西班牙裔黑人,43.8%来自有症状的患者。MG 的患病率为 16.6%(95%CI:14.9-18.5%;特定地点范围:9.9-23.5%),在圣路易斯(aPR:1.9;1.27-2.85)、格林斯伯勒(aPR:1.8;1.18-2.79)和丹佛(aPR:1.7;1.12-2.44)的患病率高于西雅图。在年龄小于 18 岁的人群中,患病率最高(30.4%),每增加 1 岁,患病率下降 3%(aPR:0.97;0.955-0.982)。MG 在尿道炎、阴道炎、宫颈炎和盆腔炎(PID)中的检出率分别为 26.8%、21.1%、11.8%和 15.4%。在无症状男性中,MG 的检出率为 9%,在无症状女性中,MG 的检出率为 15.4%,并与男性尿道炎(aPR:1.7;1.22-2.50)和衣原体感染(aPR:1.7;1.13-2.53)相关。MRM 的患病率为 59.1%(95%CI:53.1-64.8%;特定地点范围:51.3-70.6%)。MRM 与阴道炎(aPR:1.8;1.14-2.85)、宫颈炎(aPR:3.5;1.69-7.30)和 PID 宫颈炎(aPR:1.8;1.09-3.08)相关。
在有较高性传播感染风险的人群中,MG 感染很常见;对有症状的患者进行检测将有助于进行适当的治疗。大环内酯类药物耐药性很高,在没有耐药性检测的情况下,不应使用阿奇霉素。