Jefferson Francis A, Linder Brian J
Department of Urology, Mayo Clinic, Rochester, MN, USA.
Res Rep Urol. 2023 Jun 29;15:291-303. doi: 10.2147/RRU.S320684. eCollection 2023.
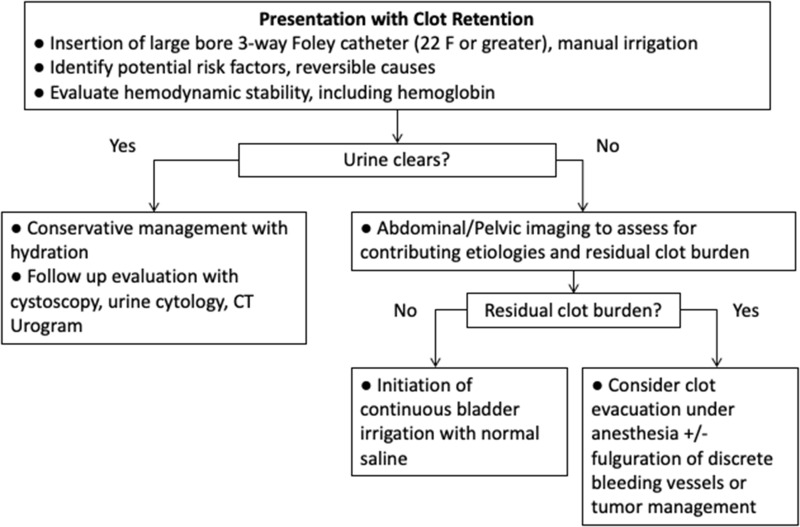
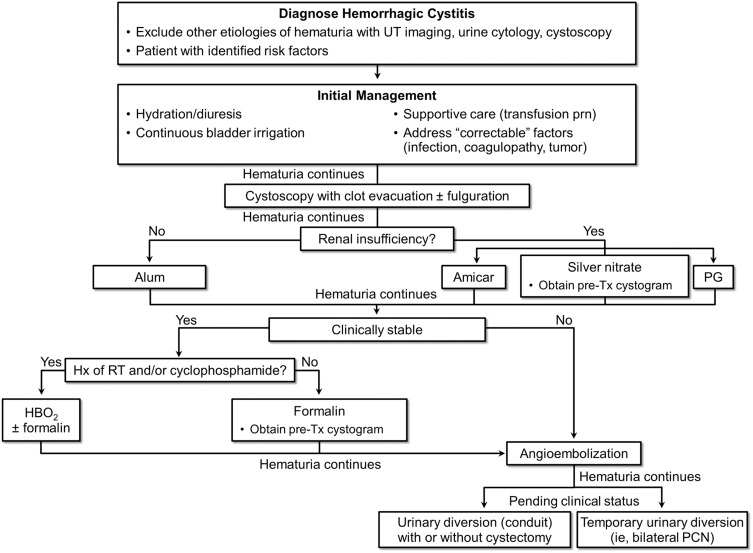
Hemorrhagic cystitis (HC) can be one of the most challenging clinical scenarios for urologists to manage. It most commonly occurs as a toxicity of pelvic radiation therapy or in patients treated with the oxazaphosphorine class of chemotherapy. Successful management of HC necessitates a stepwise approach with a thorough understanding of the various treatment options. Once ensuring hemodynamic stability, conservative management includes establishing bladder drainage, manual clot evacuation, and continuous bladder irrigation through a large-bore urethral catheter. If gross hematuria persists, operative cystoscopy with bladder clot evacuation is often required. There are multiple intravesical options for treating HC, including alum, aminocaproic acid, prostaglandins, silver nitrate, and formalin. Formalin is an intravesical option that has caustic effects on the bladder mucosa and is most often reserved as a last-line intravesical treatment. Non-intravesical management tools include hyperbaric oxygen therapy and oral pentosan polysulfate. If needed, nephrostomy tube placement or superselective angioembolization of the anterior division of the internal iliac artery can be performed. Finally, cystectomy with urinary diversion is a definitive, albeit invasive, treatment option for refractory HC. While there is no standardized algorithm, treatment modalities typically progress from less to more invasive. Clinical judgement and shared decision-making with the patient are required when choosing therapies for managing HC, as success rates are variable and some treatments may have significant or irreversible effects.
出血性膀胱炎(HC)可能是泌尿外科医生面临的最具挑战性的临床情况之一。它最常见于盆腔放射治疗的毒性反应中,或发生在接受恶唑磷类化疗的患者身上。成功管理HC需要采取循序渐进的方法,并全面了解各种治疗选择。在确保血流动力学稳定后,保守治疗包括建立膀胱引流、手动清除血块以及通过大口径尿道导管进行持续膀胱冲洗。如果肉眼血尿持续存在,通常需要进行膀胱镜检查并清除膀胱血块。治疗HC有多种膀胱内用药选择,包括明矾、氨基己酸、前列腺素、硝酸银和福尔马林。福尔马林是一种膀胱内用药,对膀胱黏膜有腐蚀作用,通常留作膀胱内治疗的最后一线选择。非膀胱内治疗工具包括高压氧治疗和口服聚多卡醇硫酸酯。如有需要,可进行肾造瘘管置入或对髂内动脉前支进行超选择性血管栓塞。最后,膀胱切除术加尿流改道术是治疗难治性HC的一种确定性治疗选择,尽管具有侵入性。虽然没有标准化的算法,但治疗方式通常从侵入性较小的逐步过渡到侵入性较大的。在选择治疗HC的方法时,需要临床判断并与患者共同决策,因为成功率各不相同,而且一些治疗可能会产生重大或不可逆的影响。