Zhang Sihui, Wang Chao, Liu Bei, Lu Qing-Bin, Shang Jia, Zhou Yihua, Jia Jidong, Xu Xiaoyuan, Rao Huiying, Han Bingfeng, Zhao Tianshuo, Chen Linyi, Xie Mingzhu, Cui Jiahao, Du Juan, Zeng Jing, Huang Ninghua, Liu Yaqiong, Zhang Lei, Zhuang Hui, Cui Fuqiang
Department of Epidemiology and Biostatistics, School of Public Health, Peking University, Beijing, 100191, PR China.
Department of Laboratorial Science and Technology, School of Public Health, Peking University, Beijing, 100191, PR China.
Lancet Reg Health West Pac. 2023 Mar 9;35:100738. doi: 10.1016/j.lanwpc.2023.100738. eCollection 2023 Jun.
China, which has the largest chronic hepatitis B virus (HBV) burden, may expand antiviral therapy to attain the World Health Organization (WHO)-2030 goal of 65% reduction in mortality. We evaluated health outcomes and cost-effectiveness of chronic HBV infection treatments based on alanine transaminase (ALT) antiviral treatment initiation thresholds and coverage in China to identify an optimal strategy.
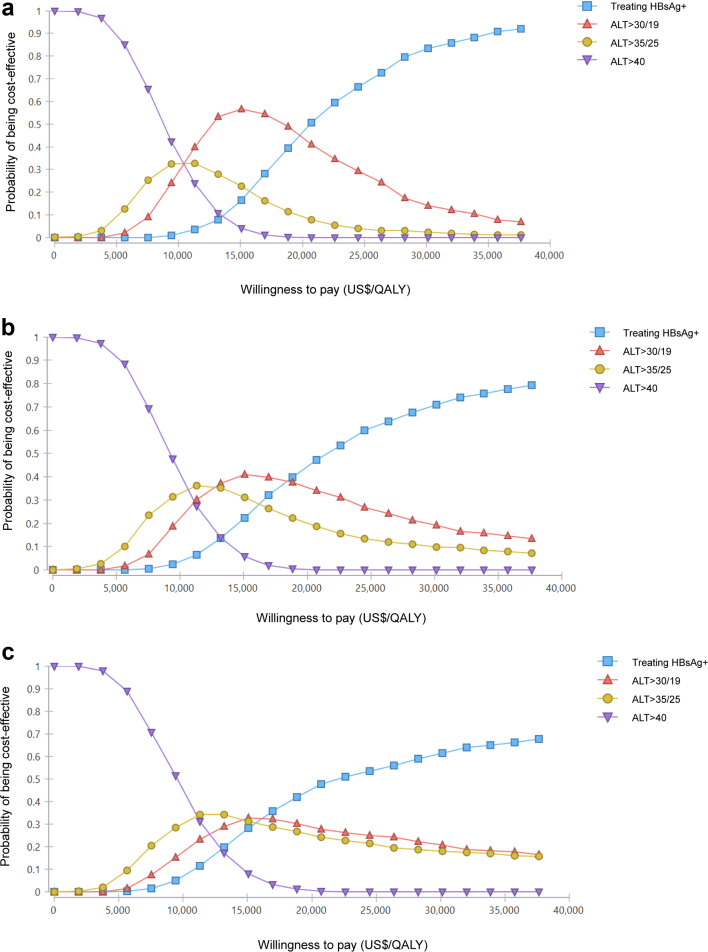
A decision-tree Markov state-transition model evaluated the cost-effectiveness of expanded antiviral treatment for chronic HBV infection by simulating 136 scenarios by ALT treatment initiation thresholds (40 U/L, 35 U/L for males and 25 U/L for females, 30 U/L for males and 19 U/L for females, and treating HBsAg+ individuals regardless of ALT values), population age groups (18-80, 30-80, and 40-80 years), implementation durations (2023, 2028, and 2033) under and treatment coverages (20%, 40%, 60%, and 80%). Deterministic and probabilistic sensitivity analyses explored model uncertainty.
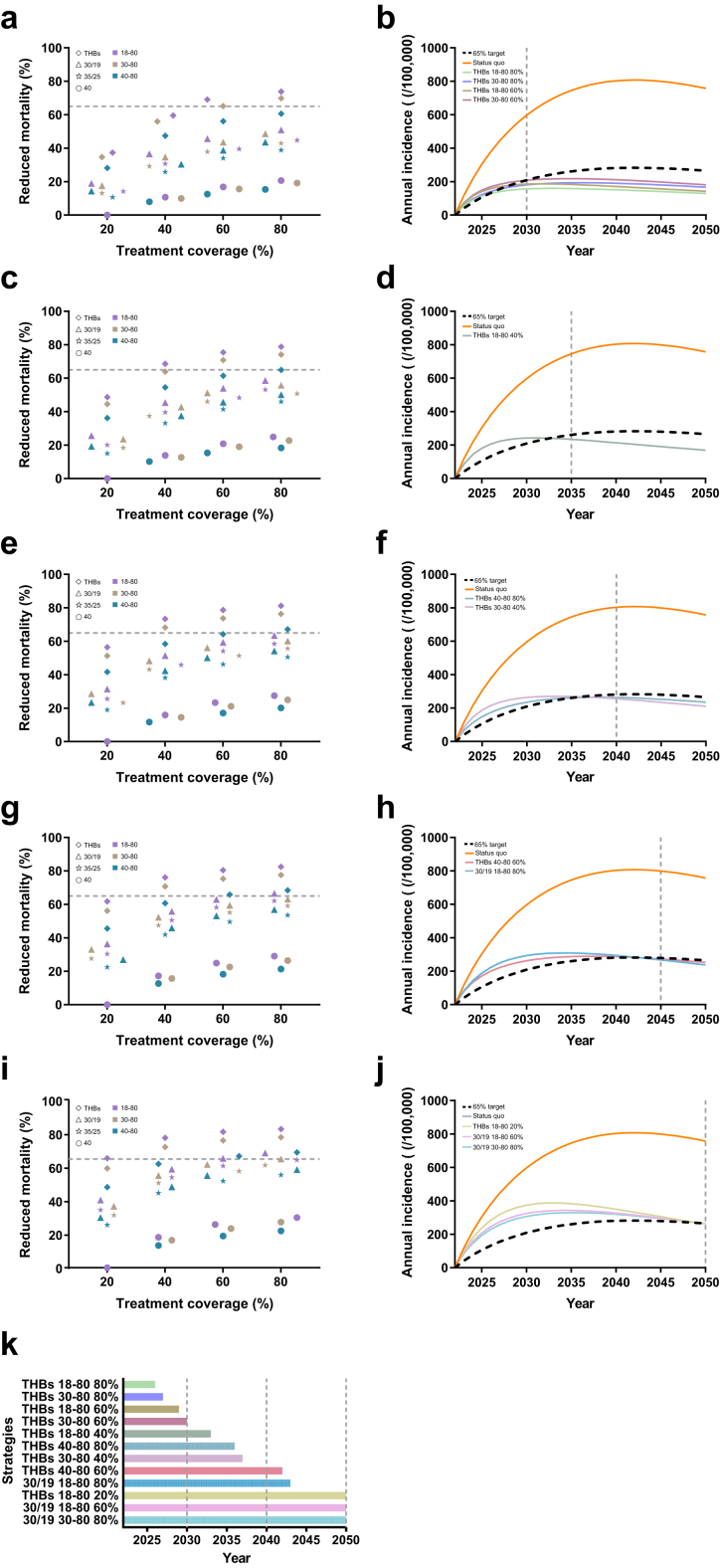
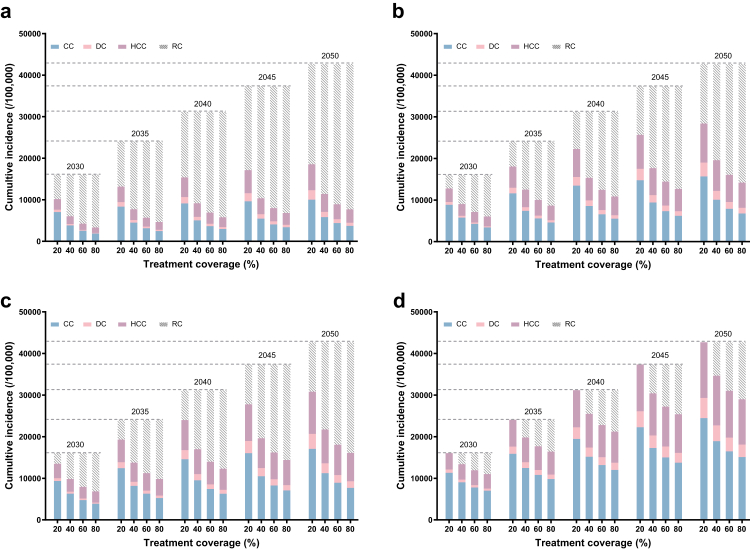
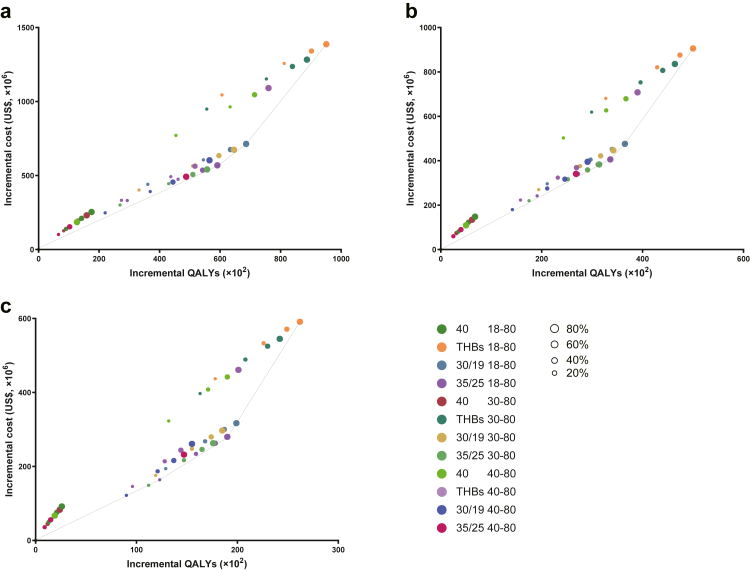
Besides the status quo, we finally simulated 135 treatment-expanding scenarios based on the cross combination of different thresholds of ALT, treatment coverages, population's age groups and implementation time. For the status quo, a cumulative incidence of 16,038-42,691 HBV-related complications and 3116-18,428 related deaths will happened between 2030 and 2050. When the treatment threshold is expanded to 'ALT > 35 in males & ALT > 25 in females' immediately without expanding treatment coverage, it will save 2554 HBV-related complications and 348 related deaths compared to the status quo among the whole cohort by 2030, and US$ 156 million more will be costed for gaining 2962 more QALYs. If we just expand the ALT threshold to ALT > 30 in males & ALT > 19 in females, 3247 HBV-related complications and 470 related deaths will be prevented by 2030 under the current treatment coverage of 20%, which will cost US$ 242 million, US$ 583 million or US$ 606 million more by the year of 2030, 2040 or 2050, respectively. Treatment expanded to HBsAg+ will save the largest number of HBV-related complications and death. This expanding strategy also results in large complications or death reduction when it is limited to patients older than 30 years or 40 years. Under this strategy, four scenarios (Treating HBsAg+ with coverage of 60% or 80% for patients older than 18 years or 30 years) showed the effectiveness in reaching the target before the year 2030. Among all the strategies, treatment expanded to HBsAg+ would cost the most while providing the highest total QALYs compared to other strategies with similar implementation scenarios. ALT thresholds of 30 U/L and 19 U/L for males and females, respectively, with 80% coverage for 18-80 years, can attain the goal by 2043.
Treating HBsAg+ individuals with 80% coverage for 18-80 years is optimal; earlier implementation of expanded antiviral treatment with a modified ALT threshold could decrease HBV-related complications and deaths to support the global target of 65% reduction in viral hepatitis B deaths.
This study was funded by Global Center for Infectious Disease and Policy Research (BMU2022XY030); Global Health and Infectious Diseases Group (BMU2022XY030); The Chinese Foundations for Hepatitis Control and Prevention (2021ZC032); National Science and Technology Project on Development Assistance for Technology, Developing China-ASEAN Public Health Research and Development Collaborating Center (KY202101004); in part by National Key R&D Program of China (2022YFC2505100).
中国是慢性乙型肝炎病毒(HBV)负担最重的国家,可能会扩大抗病毒治疗以实现世界卫生组织(WHO)到2030年将死亡率降低65%的目标。我们基于丙氨酸转氨酶(ALT)抗病毒治疗起始阈值和在中国的覆盖率,评估了慢性HBV感染治疗的健康结局和成本效益,以确定最佳策略。
一个决策树马尔可夫状态转换模型通过模拟136种情景来评估扩大慢性HBV感染抗病毒治疗的成本效益,这些情景涉及ALT治疗起始阈值(男性40 U/L、男性35 U/L且女性25 U/L、男性30 U/L且女性19 U/L,以及无论ALT值如何治疗HBsAg阳性个体)、人群年龄组(18 - 80岁、30 - 80岁和40 - 80岁)、实施持续时间(2023年、2028年和2033年)以及治疗覆盖率(20%、40%、60%和80%)。确定性和概率敏感性分析探讨了模型的不确定性。
除现状外,我们最终基于ALT不同阈值、治疗覆盖率、人群年龄组和实施时间的交叉组合模拟了135种扩大治疗的情景。对于现状,在2030年至2050年期间,将发生16,038 - 42,691例HBV相关并发症和3116 - 18,428例相关死亡。当治疗阈值立即扩大到“男性ALT > 35且女性ALT > 25”而不扩大治疗覆盖率时,到2030年,与现状相比,在整个队列中将减少2554例HBV相关并发症和348例相关死亡,并且为获得多2962个质量调整生命年(QALY)将多花费1.56亿美元。如果仅将ALT阈值扩大到男性ALT > 30且女性ALT > 19,在当前20%的治疗覆盖率下,到2030年将预防3247例HBV相关并发症和470例相关死亡,到2030年、2040年或2050年分别将多花费2.42亿美元、5.83亿美元或6.06亿美元。将治疗扩大到HBsAg阳性个体将挽救最多的HBV相关并发症和死亡。当仅限于30岁或40岁以上患者时,这种扩大策略也会导致大量并发症或死亡的减少。在该策略下,四种情景(18岁或30岁以上患者HBsAg阳性治疗覆盖率为60%或80%)显示在2030年前实现目标的有效性。在所有策略中,与具有类似实施情景的其他策略相比,将治疗扩大到HBsAg阳性个体成本最高,但提供的总QALY最高。男性和女性ALT阈值分别为30 U/L和19 U/L,18 - 80岁覆盖率为80%,到2043年可实现目标。
对18 - 80岁人群中80%的HBsAg阳性个体进行治疗是最佳方案;尽早实施基于调整后ALT阈值的扩大抗病毒治疗可减少HBV相关并发症和死亡,以支持到2030年将乙型肝炎病毒死亡减少65%的全球目标。
本研究由全球传染病与政策研究中心(BMU2022XY030);全球健康与传染病小组(BMU2022XY030);中国肝炎防治基金会(2021ZC(032));国家科技发展援助技术项目、中国 - 东盟公共卫生研发合作中心(KY202101004)资助;部分由国家重点研发计划(2022YFC2505100)资助。