Laboratory of Radiation Physics, Department of Oncology, Odense University Hospital, Kløvervænget 19, 5000 Odense, Denmark; Department of Clinical Research, University of Southern Denmark, J.B. Winsløws Vej 19.3, 5000 Odense Denmark.
Department of Radiation Oncology, Radboud University Medical Centre, P.O. Box 9101, 6500 HB Nijmegen, The Netherlands.
Radiother Oncol. 2023 Sep;186:109803. doi: 10.1016/j.radonc.2023.109803. Epub 2023 Jul 10.
The apparent diffusion coefficient (ADC), a potential imaging biomarker for radiotherapy response, needs to be reproducible before translation into clinical use. The aim of this study was to evaluate the multi-centre delineation- and calculation-related ADC variation and give recommendations to minimize it.
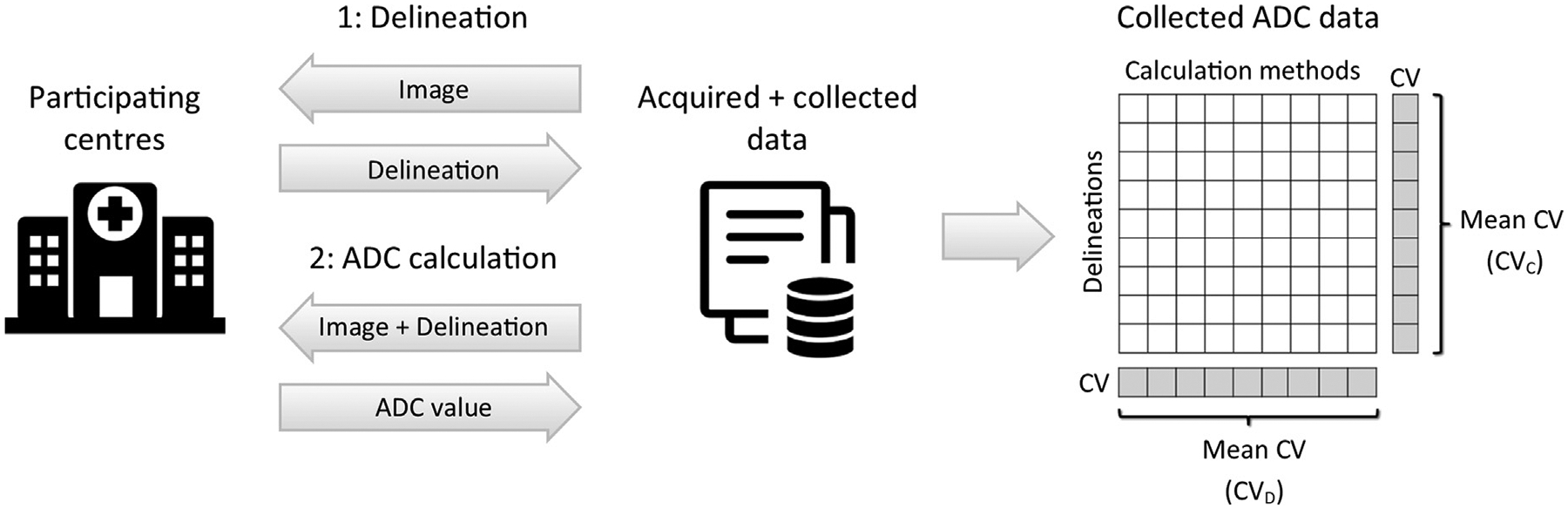
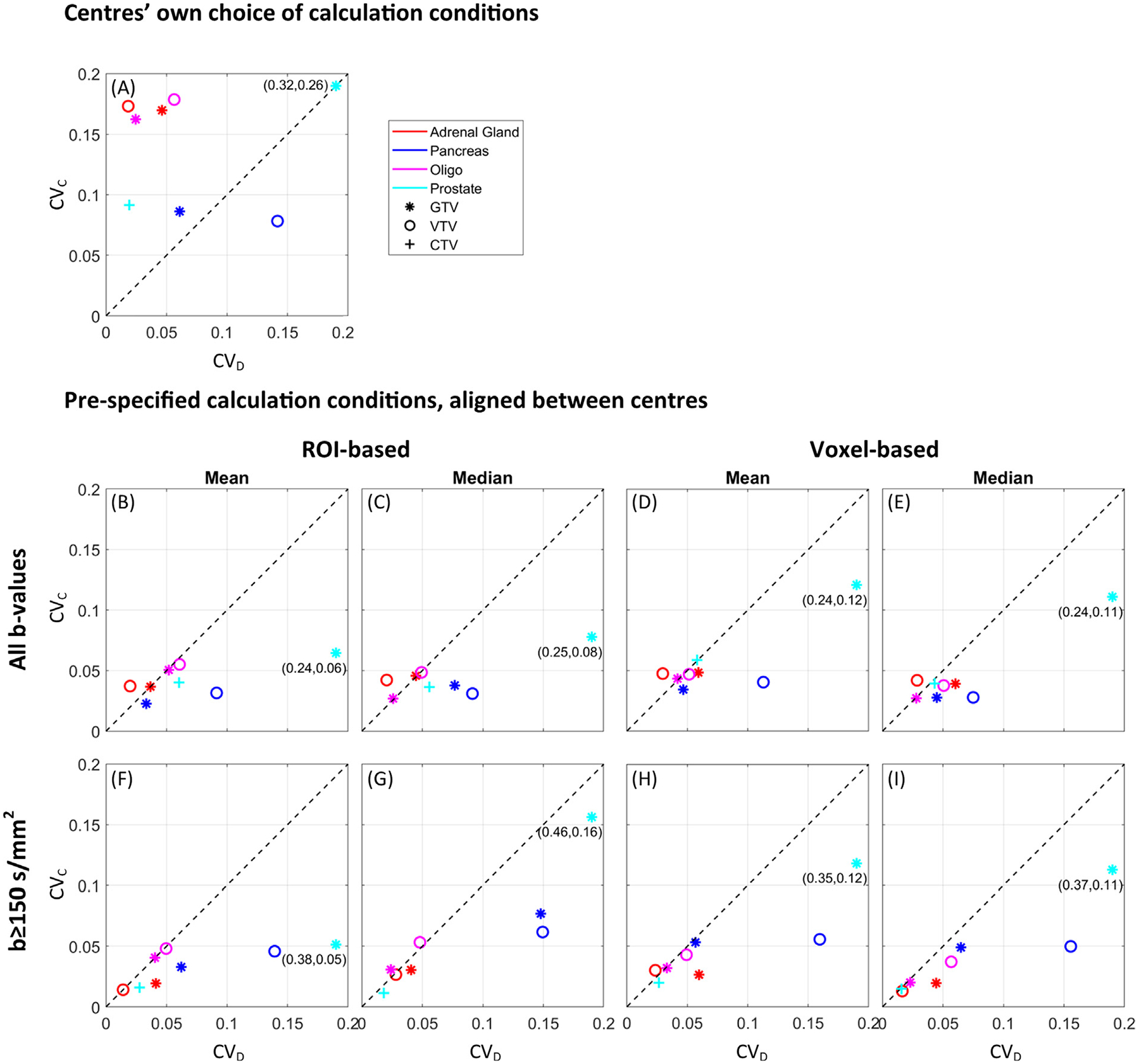
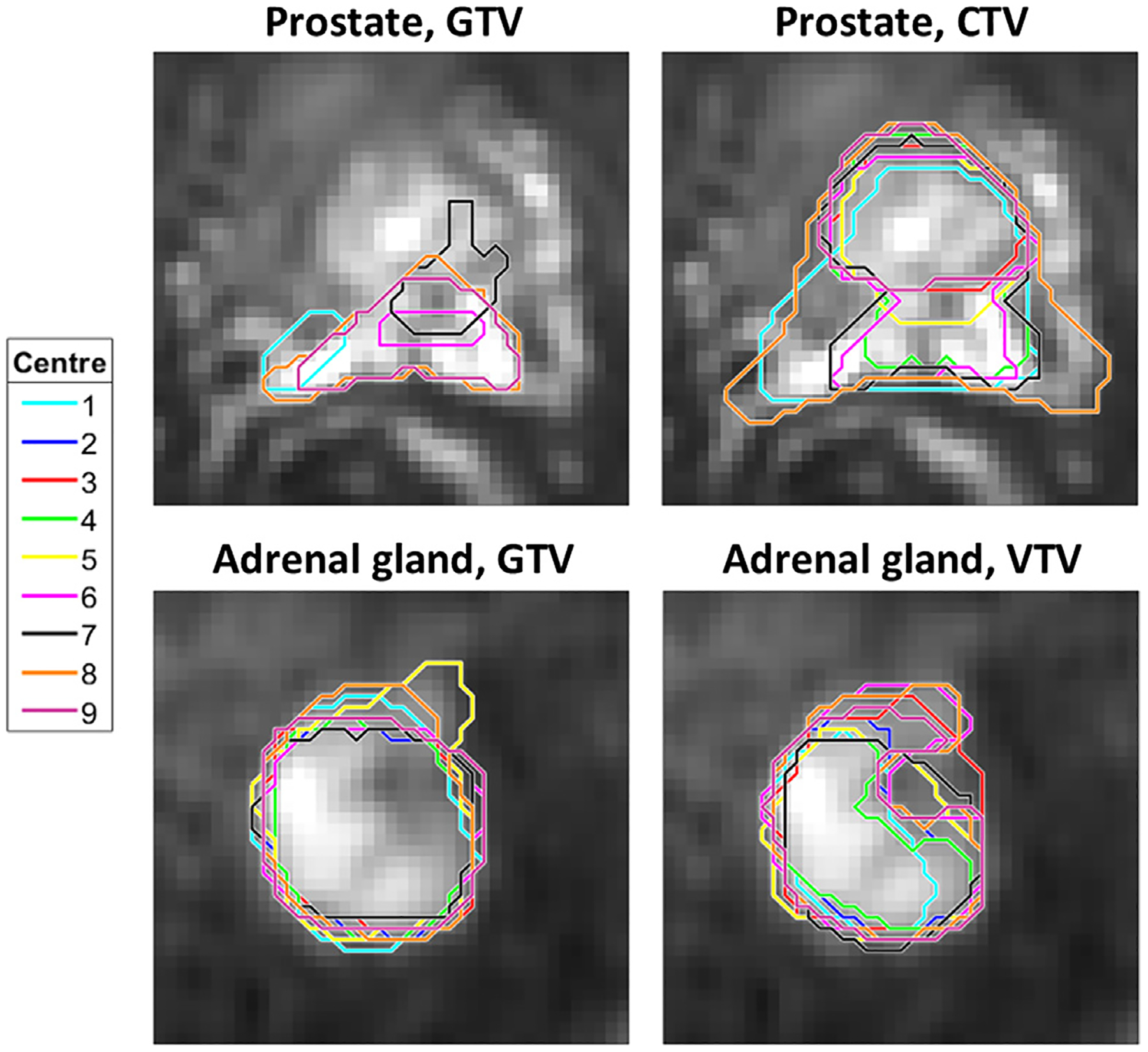
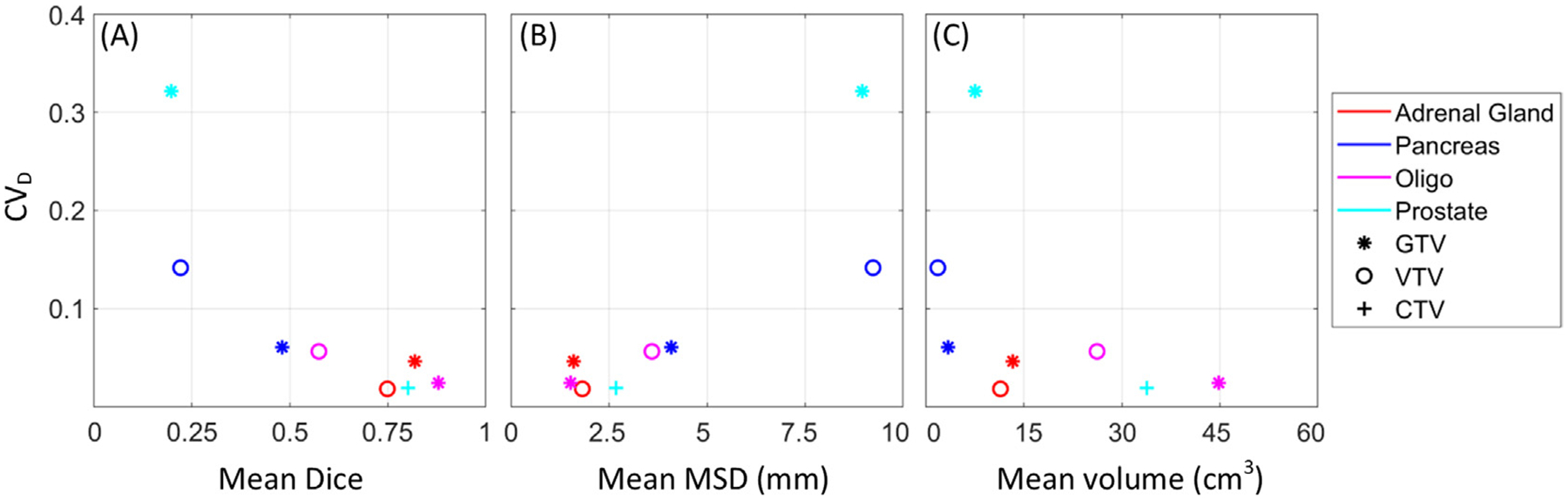
Nine centres received identical diffusion-weighted and anatomical magnetic resonance images of different cancerous tumours (adrenal gland, pelvic oligo metastasis, pancreas, and prostate). All centres delineated the gross tumour volume (GTV), clinical target volume (CTV), and viable tumour volume (VTV), and calculated ADCs using both their local calculation methods and each of the following calculation conditions: b-values 0-500 vs. 150-500 s/mm, region-of-interest (ROI)-based vs. voxel-based calculation, and mean vs. median. ADC variation was assessed using the mean coefficient of variation across delineations (CV) and calculation methods (CV). Absolute ADC differences between calculation conditions were evaluated using Friedman's test. Recommendations for ADC calculation were formulated based on observations and discussions within the Elekta MRI-linac consortium image analysis working group.
The median (range) CV and CV were 0.06 (0.02-0.32) and 0.17 (0.08-0.26), respectively. The ADC estimates differed 18% between b-value sets and 4% between ROI/voxel-based calculation (p-values < 0.01). No significant difference was observed between mean and median (p = 0.64). Aligning calculation conditions between centres reduced CV to 0.04 (0.01-0.16). CV was comparable between ROI types.
Overall, calculation methods had a larger impact on ADC reproducibility compared to delineation. Based on the results, significant sources of variation were identified, which should be considered when initiating new studies, in particular multi-centre investigations.
表观扩散系数(ADC)是一种潜在的放疗反应的影像学生物标志物,在转化为临床应用之前需要具有可重复性。本研究的目的是评估多中心勾画和计算相关 ADC 变化,并提出建议以最小化这种变化。
九个中心接收了不同癌症肿瘤(肾上腺、盆腔寡转移、胰腺和前列腺)的相同弥散加权和解剖磁共振图像。所有中心均勾画了大体肿瘤体积(GTV)、临床靶区体积(CTV)和存活肿瘤体积(VTV),并使用各自的局部计算方法和以下计算条件计算 ADC:b 值 0-500 与 150-500 s/mm、基于感兴趣区(ROI)与基于体素的计算、均值与中位数。通过勾画和计算方法的跨勾画变异系数(CV)和均值 CV 评估 ADC 变化。使用 Friedman 检验评估不同计算条件下的绝对 ADC 差异。根据 Elekta MRI-直线加速器联盟图像分析工作组的观察和讨论,制定了 ADC 计算建议。
中位(范围)CV 和 CV 分别为 0.06(0.02-0.32)和 0.17(0.08-0.26)。b 值集之间的 ADC 估计值差异为 18%,ROI/体素计算之间的差异为 4%(p 值均小于 0.01)。均值和中位数之间无显著差异(p=0.64)。中心之间的计算条件对齐将 CV 降低至 0.04(0.01-0.16)。ROI 类型之间的 CV 相似。
总体而言,与勾画相比,计算方法对 ADC 重现性的影响更大。基于这些结果,确定了显著的变异来源,在启动新研究时,特别是在多中心研究时,应考虑这些来源。