Cartes Rodrigo, Karim Muneeb Uddin, Tisseverasinghe Steven, Tolba Marwan, Bahoric Boris, Anidjar Maurice, McPherson Victor, Probst Stephan, Rompré-Brodeur Alexis, Niazi Tamim
Department of Radiation Oncology, McGill University, Montreal, QC H3A 0G4, Canada.
Department of Radiation Oncology, McGill University, Gatineau, QC J8V 3R2, Canada.
Cancers (Basel). 2023 Jun 27;15(13):3363. doi: 10.3390/cancers15133363.
There is an ongoing debate on the optimal sequencing of androgen deprivation therapy (ADT) and radiotherapy (RT) in patients with localized prostate cancer (PCa). Recent data favors concurrent ADT and RT over the neoadjuvant approach.
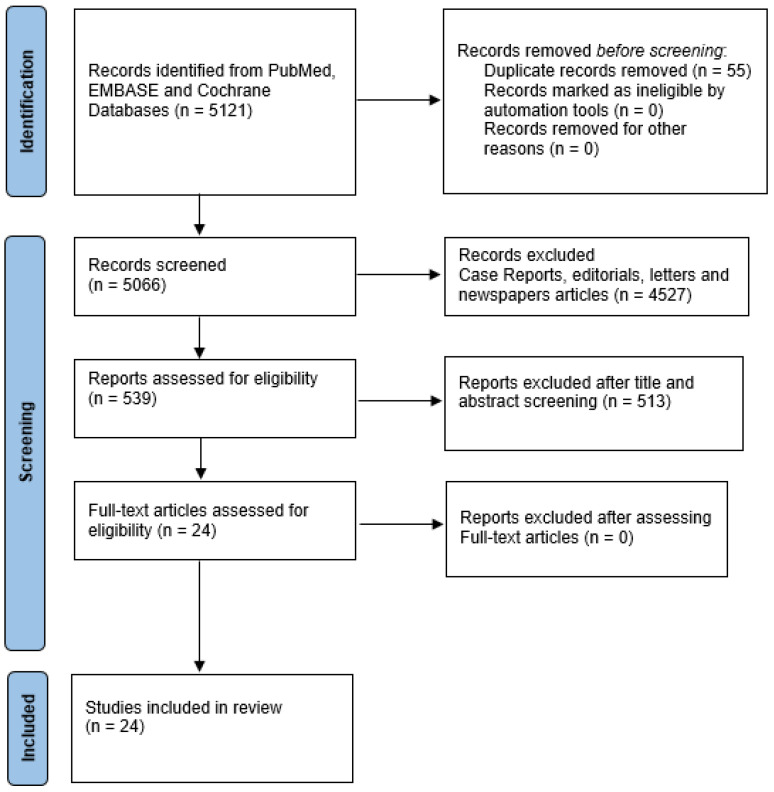
We conducted a systematic review in PubMed, EMBASE, and Cochrane Databases assessing the combination and optimal sequencing of ADT and RT for Intermediate-Risk (IR) and High-Risk (HR) PCa.
Twenty randomized control trials, one abstract, one individual patient data meta-analysis, and two retrospective studies were selected. HR PCa patients had improved survival outcomes with RT and ADT, particularly when a long-course Neoadjuvant-Concurrent-Adjuvant ADT was used. This benefit was seen in IR PCa when adding short-course ADT, although less consistently. The best available evidence indicates that concurrent over neoadjuvant sequencing is associated with better metastases-free survival at 15 years. Although most patients had IR PCa, HR participants may have been undertreated with short-course ADT and the absence of pelvic RT. Conversely, retrospective data suggests a survival benefit when using the neoadjuvant approach in HR PCa patients.
The available literature supports concurrent ADT and RT initiation for IR PCa. Neoadjuvant-concurrent-adjuvant sequencing should remain the standard approach for HR PCa and is an option for IR PCa.
对于局限性前列腺癌(PCa)患者,雄激素剥夺疗法(ADT)和放疗(RT)的最佳顺序仍存在争议。近期数据表明,与新辅助治疗方法相比,同步进行ADT和RT更具优势。
我们在PubMed、EMBASE和Cochrane数据库中进行了一项系统评价,评估ADT和RT联合应用以及针对中危(IR)和高危(HR)PCa的最佳顺序。
共入选了20项随机对照试验、1篇摘要、1项个体患者数据荟萃分析和2项回顾性研究。HR PCa患者接受RT和ADT治疗后生存结局有所改善,尤其是采用长疗程新辅助-同步-辅助ADT时。在IR PCa患者中,添加短疗程ADT时也观察到了这种益处,尽管不太一致。现有最佳证据表明,与新辅助治疗顺序相比,同步治疗顺序与15年无转移生存率更高相关。虽然大多数患者为IR PCa,但HR患者可能因接受短疗程ADT且未进行盆腔RT而治疗不足。相反,回顾性数据表明,HR PCa患者采用新辅助治疗方法时具有生存获益。
现有文献支持IR PCa患者同步开始ADT和RT。新辅助-同步-辅助顺序应仍然是HR PCa的标准治疗方法,也是IR PCa的一种选择。