Department of Internal Medicine, Faculty of Medicine, Grigore T. Popa University of Medicine and Pharmacy of Iasi, 16 University Street, 700115 Iasi, Romania.
Prof. Dr. George I.M. Georgescu Institute of Cardiovascular Diseases, Carol I Boulevard, No. 50, 700503 Iasi, Romania.
Int J Mol Sci. 2023 Jun 22;24(13):10510. doi: 10.3390/ijms241310510.
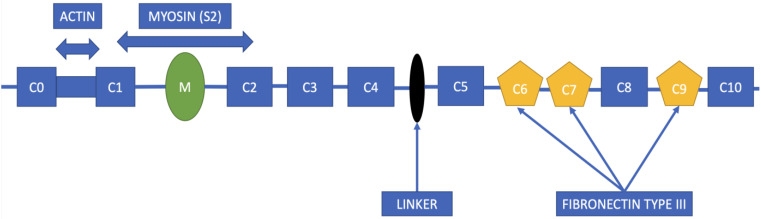
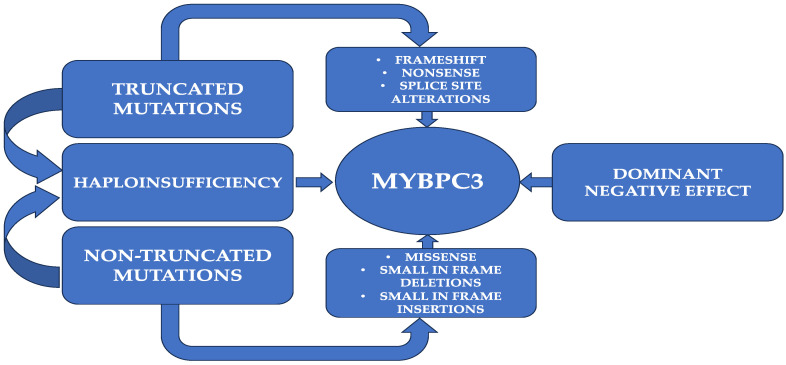
Hypertrophic cardiomyopathy (HCM) is the most prevalent genetically inherited cardiomyopathy that follows an autosomal dominant inheritance pattern. The majority of HCM cases can be attributed to mutation of the MYBPC3 gene, which encodes cMyBP-C, a crucial structural protein of the cardiac muscle. The manifestation of HCM's morphological, histological, and clinical symptoms is subject to the complex interplay of various determinants, including genetic mutation and environmental factors. Approximately half of MYBPC3 mutations give rise to truncated protein products, while the remaining mutations cause insertion/deletion, frameshift, or missense mutations of single amino acids. In addition, the onset of HCM may be attributed to disturbances in the protein and transcript quality control systems, namely, the ubiquitin-proteasome system and nonsense-mediated RNA dysfunctions. The aforementioned genetic modifications, which appear to be associated with unfavorable lifelong outcomes and are largely influenced by the type of mutation, exhibit a unique array of clinical manifestations ranging from asymptomatic to arrhythmic syncope and even sudden cardiac death. Although the current understanding of the MYBPC3 mutation does not comprehensively explain the varied phenotypic manifestations witnessed in patients with HCM, patients with pathogenic MYBPC3 mutations can exhibit an array of clinical manifestations ranging from asymptomatic to advanced heart failure and sudden cardiac death, leading to a higher rate of adverse clinical outcomes. This review focuses on MYBPC3 mutation and its characteristics as a prognostic determinant for disease onset and related clinical consequences in HCM.
肥厚型心肌病(HCM)是最常见的遗传性心脏病,呈常染色体显性遗传模式。大多数 HCM 病例可归因于 MYBPC3 基因突变,该基因编码 cMyBP-C,是心肌的重要结构蛋白。HCM 的形态、组织学和临床症状的表现受到各种决定因素的复杂相互作用的影响,包括基因突变和环境因素。大约一半的 MYBPC3 突变导致截短的蛋白产物,而其余的突变导致单个氨基酸的插入/缺失、移码或错义突变。此外,HCM 的发作可能归因于蛋白质和转录质量控制系统的紊乱,即泛素-蛋白酶体系统和无意义介导的 RNA 功能障碍。上述遗传改变似乎与不利的终身结局有关,并且在很大程度上受到突变类型的影响,表现出从无症状到心律失常性晕厥甚至心脏性猝死的独特临床表现。尽管目前对 MYBPC3 突变的理解不能全面解释 HCM 患者所见的各种表型表现,但具有致病性 MYBPC3 突变的患者可表现出从无症状到晚期心力衰竭和心脏性猝死的一系列临床表现,导致不良临床结局的发生率更高。本综述重点关注 MYBPC3 突变及其作为疾病发生和相关临床后果的预后决定因素的特征。