Rao C Mohan, Mohapatra Amrut Kumar, Patnaik Aswini Kumar, Panda Prem S, Behera Prasanta Ranjan
Department of Pulmonary Medicine, Kalinga Institute of Medical Sciences Bhubaneswar, Odisha, India.
Department of Nephrology, Kalinga Institute of Medical Sciences Bhubaneswar, Odisha, India.
J Family Med Prim Care. 2023 May;12(5):971-978. doi: 10.4103/jfmpc.jfmpc_1853_22. Epub 2023 May 31.
COVID-19 pandemic hit Odisha province from April 2020 to December 2020, then from April 2021 to August 2021 and from February 2022 to April 2022 as the first, second, and third waves, respectively, with the most severe form witnessed during the second wave. Kalinga Institute of Medical Sciences hospital in Odisha was declared a Dedicated COVID Hospital (DCH) during those three waves and witnessed 9485 cases of admissions among which there were 1214 deaths. COVAXIN vaccination of the vulnerable population was launched in February 2021 onwards. This study has been done to know the clinic-biochemical profiles, radiologic findings of COVID-19 admitted patients, the predictors of mortality in the second wave, and clinical outcomes in the three waves in relation to COVAXIN vaccination status.
This was a serial three-round retrospective study from the electronic medical records using multistage random sampling where we collected and critically analyzed the demographic, and all the relevant possible health data of the cases that consist of 514 cases admitted in three waves. The data from death certificates among the 555 cases in the second wave have been analyzed to conclude predictors of mortality.
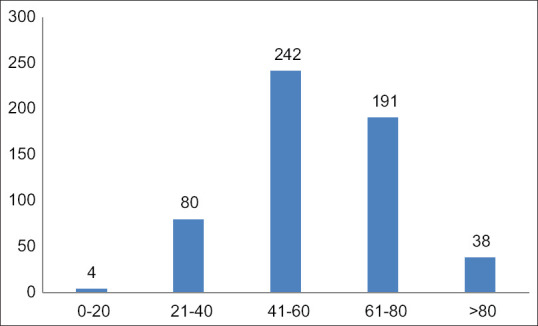
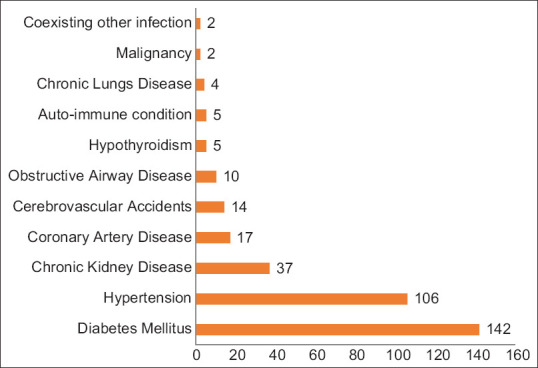
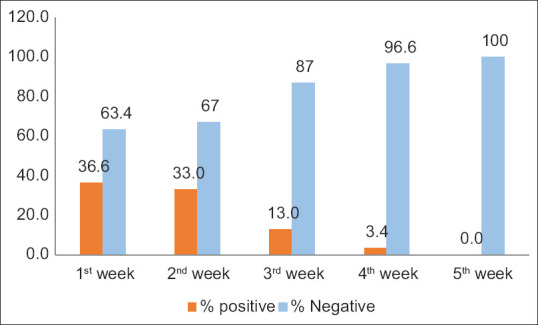
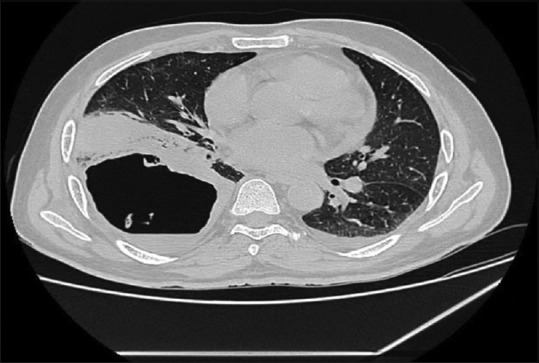
Mortality increased with age, male gender, comorbidities, and raised C-reactive protein level. High NL ratio, extent of pulmonary involvement. There was a wide variation in incidence and spectrum of illness starting from 79% incidence of mild symptomatic in the initial and third wave, but remained in the range of 35-65% in the second wave, respectively, and the most noticeable symptomatic illness was that of the upper respiratory tract. In fulminant cases, the mode of presentations was severe pneumonia and acute respiratory distress syndrome. Males were more sufferers than females. Children had better outcomes compared to adults. COVID-associated coagulopathy had a normal platelet count. Subsequently, in 2021 year onwards vaccination of the vulnerable population was launched in a phased manner that changed the dynamics of the disease outcome by better survival chances despite intercurrent COVID infection by induction of herd immunity. On the contrary, there was a higher prevalence of serious illness among non-vaccinated individuals. While the cases continued during the second wave of the pandemic, long COVID became a clinical entity of symptomatic that persisted or recurred among the COVID illness recovered cases after reverse transcriptase polymerase chain reaction results for COVID-19 became negative. The symptoms consisted of fatigue, cough, dyspnea as pulmonary manifestations and extra-pulmonary involvement of the cardiac, renal, and central nervous systems and the pulmonary imaging features consisted of interstitial pneumonia, consolidation, cavity pattern, and prone to microbial infection. These events lead to morbidity and admission. Coinciding with the vaccination of all population of Odisha province with the first dose of the vaccine by around the period of the first quarter of 2022, there was a new variant named Omicron responsible in the third wave, in which the majority of the admitted cases had.mild upper respiratory illness. This was not as lethal as its predecessors due to its lower propensity to invade the lungs and blood vessels.
Immune dysregulation plays a central role in the pathogenesis of the manifestations. Vaccine-induced protection and the induction of herd immunity played a proactive role in the waning of the severity of clinical presentations.
2020年4月至2020年12月、2021年4月至2021年8月以及2022年2月至2022年4月,新冠疫情分别以第一波、第二波和第三波的形式袭击了奥里萨邦,其中第二波最为严重。在这三波疫情期间,奥里萨邦的卡林加医学科学研究所医院被宣布为新冠定点医院(DCH),共收治了9485例患者,其中1214例死亡。2021年2月起开始对易感人群进行科维沙欣疫苗接种。本研究旨在了解新冠确诊患者的临床生化特征、影像学表现、第二波疫情中死亡的预测因素以及三波疫情中与科维沙欣疫苗接种状况相关的临床结局。
这是一项采用多阶段随机抽样的三轮回顾性系列研究,从电子病历中收集并严格分析了三波疫情中收治的514例病例的人口统计学资料及所有相关的可能健康数据。对第二波疫情中555例病例的死亡证明数据进行分析,以得出死亡的预测因素。
死亡率随年龄、男性性别、合并症以及C反应蛋白水平升高而增加。中性粒细胞与淋巴细胞比值高、肺部受累程度高。发病率和疾病谱差异很大,初始波和第三波中轻症症状的发病率为79%,但第二波中分别保持在35%-65%的范围内,最明显的症状性疾病是上呼吸道疾病。在暴发性病例中,表现形式为重症肺炎和急性呼吸窘迫综合征。男性患者多于女性。儿童的预后优于成人。新冠相关凝血病患者血小板计数正常。随后,从2021年起,易感人群开始分阶段接种疫苗,通过诱导群体免疫,尽管在感染新冠期间仍有并发感染,但更好的生存机会改变了疾病结局的动态变化。相反,未接种疫苗的个体中重症患病率更高。在第二波疫情期间病例仍在持续,在新冠疾病康复病例中,新冠病毒逆转录聚合酶链反应结果呈阴性后,长期新冠成为一种有症状的临床实体,持续存在或复发。症状包括疲劳、咳嗽、呼吸困难等肺部表现以及心脏、肾脏和中枢神经系统的肺外受累,肺部影像学特征包括间质性肺炎、实变、空洞形成,且易发生微生物感染。这些情况导致发病和住院。大约在2022年第一季度期间,奥里萨邦全体人口接种了第一剂疫苗,与此同时,出现了一种名为奥密克戎的新变种,引发了第三波疫情,其中大多数入院病例患有轻度上呼吸道疾病。由于其侵袭肺部和血管的倾向较低,其致死性不如之前的变种。
免疫失调在临床表现的发病机制中起核心作用。疫苗诱导的保护作用和群体免疫的诱导在减轻临床症状严重程度方面发挥了积极作用。