Department of Gastroenterology, Hepatology, and Nutrition, The University of Texas MD Anderson Cancer Center, Houston, TX, USA.
Epidemiology and screening unit, Centro di Riferimento per l'Epidemiologia e la Prevenzione Oncologica in Piemonte, Turin, Italy.
Gut. 2023 Oct;72(10):1904-1918. doi: 10.1136/gutjnl-2023-329701. Epub 2023 Jul 18.
New screening tests for colorectal cancer (CRC) are rapidly emerging. Conducting trials with mortality reduction as the end point supporting their adoption is challenging. We re-examined the principles underlying evaluation of new non-invasive tests in view of technological developments and identification of new biomarkers.
A formal consensus approach involving a multidisciplinary expert panel revised eight previously established principles.
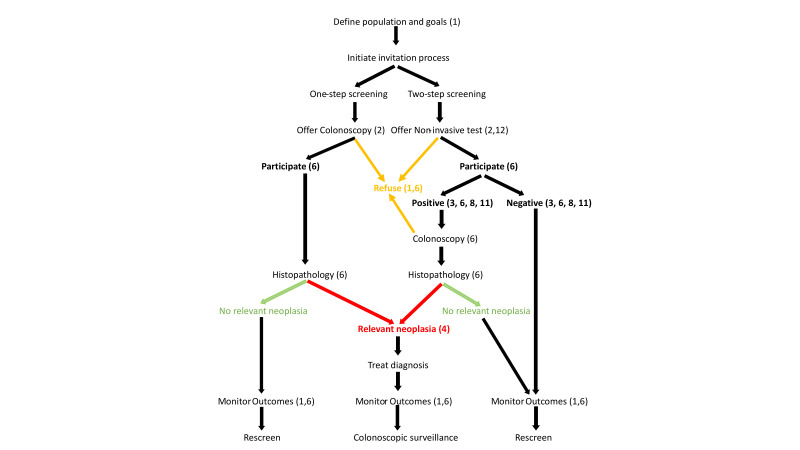
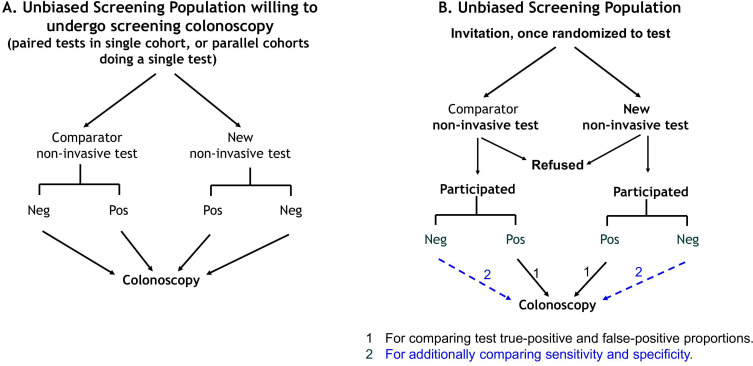
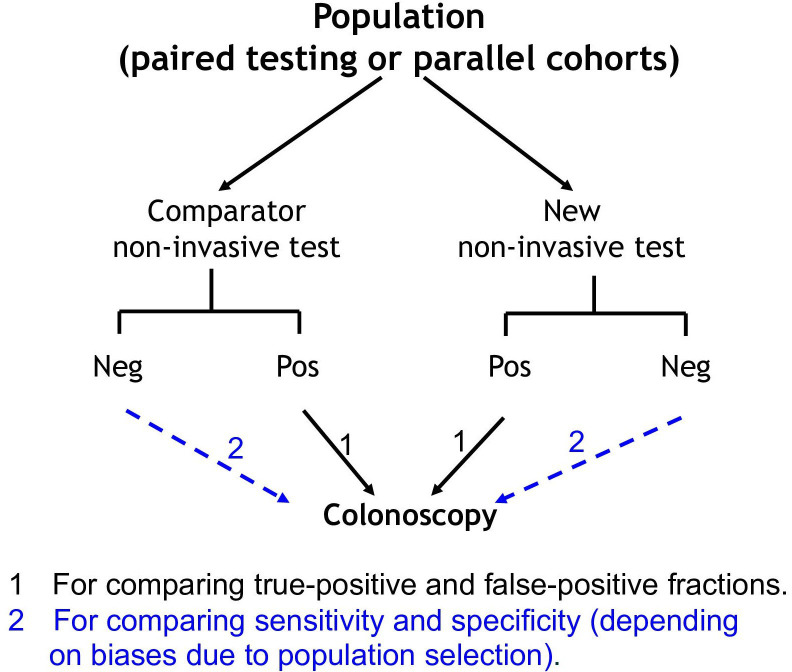
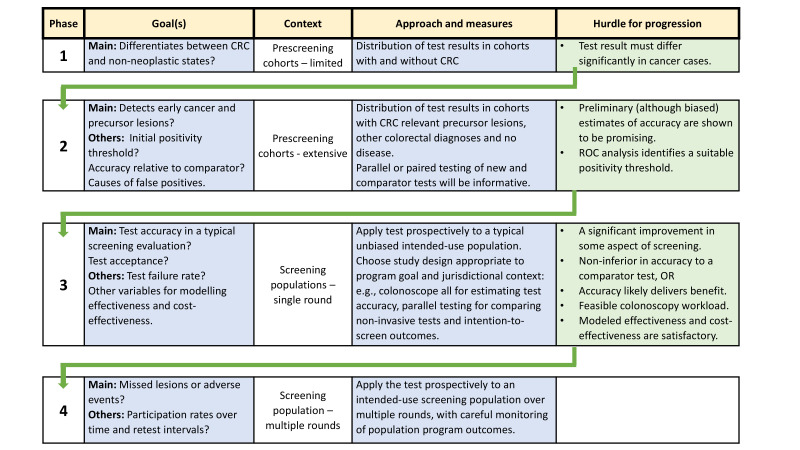
Twelve newly stated principles emerged. Effectiveness of a new test can be evaluated by comparison with a proven comparator non-invasive test. The faecal immunochemical test is now considered the appropriate comparator, while colonoscopy remains the diagnostic standard. For a new test to be able to meet differing screening goals and regulatory requirements, flexibility to adjust its positivity threshold is desirable. A rigorous and efficient four-phased approach is proposed, commencing with small studies assessing the test's ability to discriminate between CRC and non-cancer states (), followed by prospective estimation of accuracy across the continuum of neoplastic lesions in neoplasia-enriched populations (). If these show promise, a provisional test positivity threshold is set before evaluation in typical screening populations. prospective studies determine single round intention-to-screen programme outcomes and confirm the test positivity threshold. studies involve evaluation over repeated screening rounds with monitoring for missed lesions. Phases III and IV findings will provide the real-world data required to model test impact on CRC mortality and incidence.
New non-invasive tests can be efficiently evaluated by a rigorous phased comparative approach, generating data from unbiased populations that inform predictions of their health impact.
结直肠癌(CRC)的新型筛查检测方法层出不穷。以降低死亡率为终点开展临床试验以支持其应用具有挑战性。我们根据技术发展和新生物标志物的发现,重新审视了评估新型非侵入性检测方法的基本原则。
一个多学科专家小组采用正式的共识方法修订了之前确立的八项原则。
提出了 12 项新原则。可通过与已证实的非侵入性对照检测进行比较来评估新检测方法的有效性。粪便免疫化学检测现在被认为是合适的对照检测,而结肠镜检查仍然是诊断标准。为了使新检测能够满足不同的筛查目标和监管要求,期望其阳性阈值具有灵活性以进行调整。建议采用严格和高效的四阶段方法,首先进行小型研究以评估检测区分 CRC 和非癌症状态的能力(),然后在富含肿瘤的人群中对肿瘤病变连续体进行准确性的前瞻性估计()。如果这些研究有前景,则在典型的筛查人群中评估之前设置暂定的检测阳性阈值。前瞻性研究确定单次意向筛查计划的结果,并确认检测阳性阈值。研究涉及多次筛查轮次的评估,并监测遗漏的病变。第三和第四阶段的研究结果将提供建模检测对 CRC 死亡率和发病率影响所需的真实世界数据。
新型非侵入性检测方法可以通过严格的分阶段比较方法进行有效评估,从无偏倚人群中获取数据,从而预测其对健康的影响。