Buchwald Zoltan, Vempati Amrita
Creighton University School of Medicine Phoenix Program, Maricopa Medical Center, Department of Emergency Medicine, Phoenix, AZ.
J Educ Teach Emerg Med. 2020 Jul 15;5(3):S1-S27. doi: 10.21980/J8ZP86. eCollection 2020 Jul.
This scenario was developed to educate junior and senior emergency medicine (EM) residents.
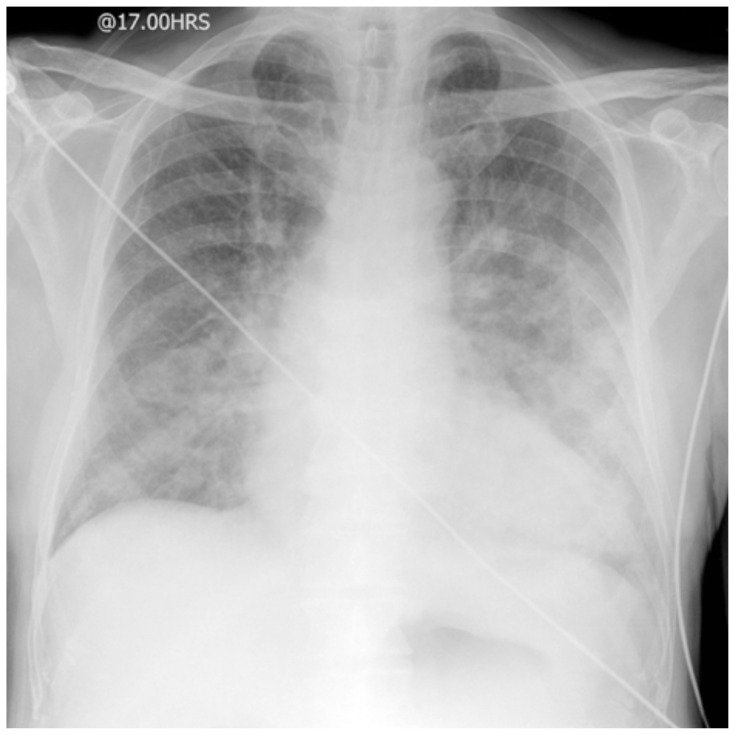
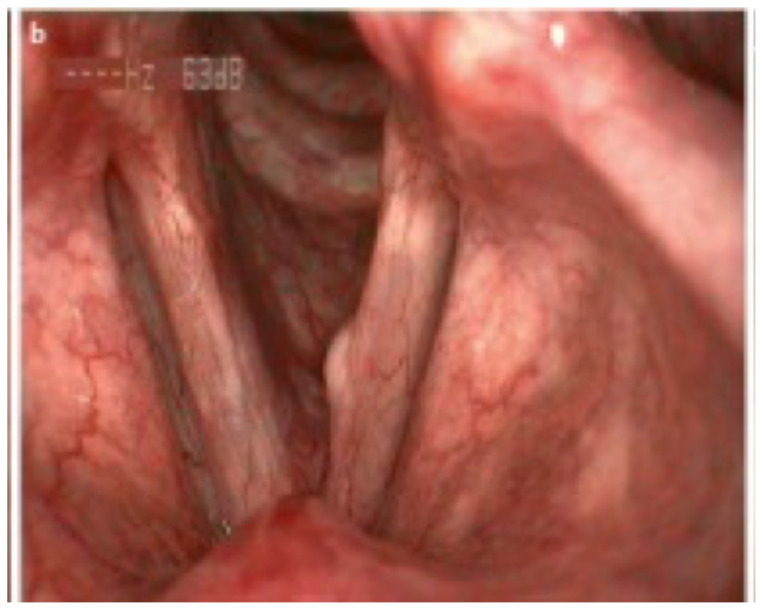
EM Model of Practice recommends that the residents are able to manage patients in a critical condition from massive hemoptysis. Mild to moderate hemoptysis can be self-limiting and often can be managed with conservative measures; however, massive hemoptysis is a life-threatening emergency that needs to be managed promptly. Mortality from massive hemoptysis is about 13%-18%.1 There are several causes for hemoptysis ranging from pulmonary to vascular causes. Diffuse alveolar hemorrhage (DAH) causes hemoptysis only 0.2% which makes it a very rare but devastating disease.2 Hemoptysis from DAH can present a significant challenge to an EM physician since it can present in various ways including chest pain, shortness of breath or hemoptysis. Up to 40% of the patients can present without hemoptysis which makes it a diagnostic dilemma.3 Patients presenting with massive hemoptysis from DAH require management for hypovolemic shock, hypoxic respiratory arrest and potential cardiac arrest. The physicians also need to perform adequate ventilator management to help with alveolar recruitment. This simulation case can help discuss some of the nuances of the management of hemoptysis and DAH.
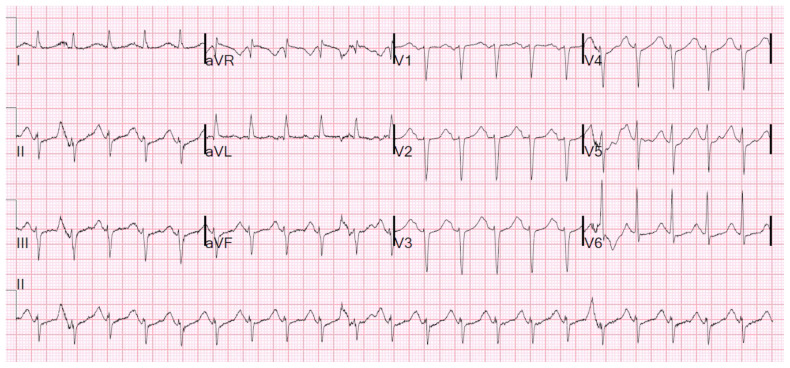
By the end of this simulation session, learners will be able to: (1) recognize worsening respiratory status of a patient with hemoptysis and intervene appropriately, (2) manage a patient with severe hemoptysis and perform appropriate ventilator management, (3) manage sinus tachycardia with QT prolongation on the ECG caused by cocaine and hypomagnesemia, (4) address various etiologies of hemoptysis, (5) discuss the causes of massive hemoptysis and management options, and (6) review ventilation strategies in an intubated hypoxic patient.
This session was conducted using high-fidelity simulation, which was immediately followed by an in-depth debriefing session. Each session had 3 EM residents from various levels of training on the team and 7 observers. There was 1 simulation instructor running the session and 1 simulation technician who acted as a nurse.
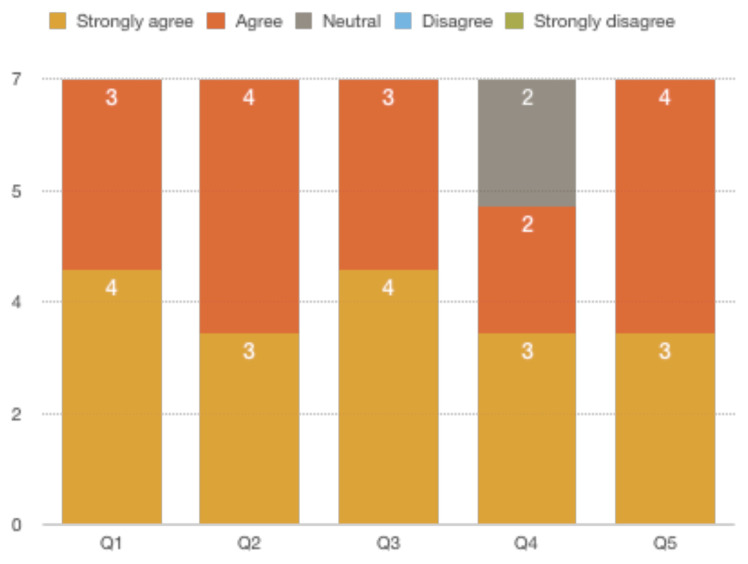
After the simulation and debriefing session was complete, an online survey was sent via surveymonkey.com to all the participants. The survey collected responses to the following questions: (1) the case was believable, (2) the case had right amount of complexity, (3) the case helped in improving medical knowledge and patient care, (4) the simulation environment gave me a real-life experience and, (5) the debriefing session after simulation helped improve my knowledge. A Likert scale was used to collect the responses.
Seven learners responded to the survey. One hundred percent of them either agreed or strongly agreed that the case was beneficial in learning and improving patient care. They also agreed that it helped in improving medical knowledge. The post-session debrief was found to be very helpful by all the learners.
High-fidelity simulation was a cost-effective yet realistic way to manage severe hemoptysis, PEA (pulseless electrical activity), and persistent hypoxia in patients with diffuse alveolar hemorrhage. Starting the case with severe hypoxia that quickly progresses to PEA helps the learner to manage the patient quickly and effectively. Overall, learners enjoyed managing the patient, followed by discussing the various management strategies.
Hemoptysis, diffuse alveolar hemorrhage, medical simulation, respiratory.
本病例场景旨在培训急诊医学(EM)专业的低年资和高年资住院医师。
急诊医学实践模式建议住院医师能够处理大量咯血导致的危急情况。轻度至中度咯血通常可自行缓解,往往可采用保守措施处理;然而,大量咯血是危及生命的紧急情况,需要迅速处理。大量咯血的死亡率约为13% - 18%。咯血的病因有多种,从肺部到血管性病因都有。弥漫性肺泡出血(DAH)导致咯血的情况仅占0.2%,这使其成为一种非常罕见但极具破坏性的疾病。DAH引起的咯血对急诊医师来说是一项重大挑战,因为其表现形式多样,包括胸痛、呼吸急促或咯血。高达40%的患者可能无咯血表现,这使其诊断成为难题。因DAH出现大量咯血的患者需要处理低血容量性休克、低氧性呼吸骤停以及潜在的心搏骤停。医师还需要进行适当的通气管理以促进肺泡复张。本模拟病例有助于探讨咯血和DAH处理中的一些细微差别。
在本次模拟课程结束时,学习者应能够:(1)识别咯血患者不断恶化的呼吸状况并进行适当干预;(2)处理严重咯血患者并进行适当的通气管理;(3)处理由可卡因和低镁血症导致心电图QT间期延长的窦性心动过速;(4)应对咯血的各种病因;(5)讨论大量咯血的病因及处理方法;(六)复习插管低氧患者的通气策略。
本次课程采用高保真模拟,随后立即进行深入的总结汇报。每次课程团队中有3名处于不同培训阶段的急诊医学住院医师和7名观察员。有1名模拟教员主持课程,1名模拟技术员扮演护士。
模拟和总结汇报课程结束后,通过surveymonkey.com向所有参与者发送在线调查问卷。该调查收集对以下问题的回答:(1)病例是否可信;(2)病例的复杂程度是否合适;(3)病例是否有助于提高医学知识和患者护理水平;(4)模拟环境是否给人真实的体验;(5)模拟后的总结汇报课程是否有助于提高知识水平。采用李克特量表收集回答。
7名学习者回复了调查问卷。他们百分之百地同意或强烈同意该病例对学习和改善患者护理有益。他们还同意该病例有助于提高医学知识。所有学习者都认为课后的总结汇报非常有帮助。
高保真模拟是处理弥漫性肺泡出血患者严重咯血、心脏停搏(无脉电活动)和持续性低氧的一种经济有效且逼真的方法。以迅速进展为心脏停搏(无脉电活动)的严重低氧开始病例,有助于学习者快速有效地处理患者。总体而言,学习者喜欢处理该病例,随后讨论各种处理策略。
咯血、弥漫性肺泡出血、医学模拟、呼吸