Department of Neurology, The Ohio State University, Columbus, Ohio; Health Services Research Program, Department of Neurology, University of Michigan, Ann Arbor, Michigan.
Health Services Research Program, Department of Neurology, University of Michigan, Ann Arbor, Michigan.
J Pain. 2023 Dec;24(12):2268-2282. doi: 10.1016/j.jpain.2023.07.011. Epub 2023 Jul 17.
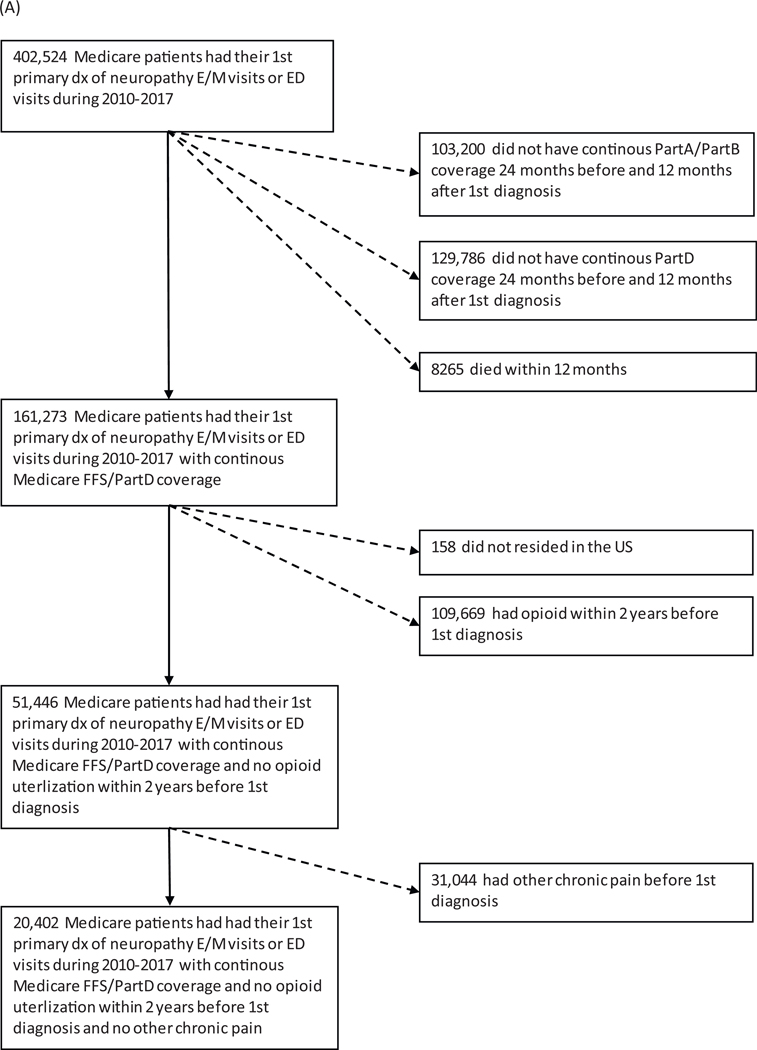
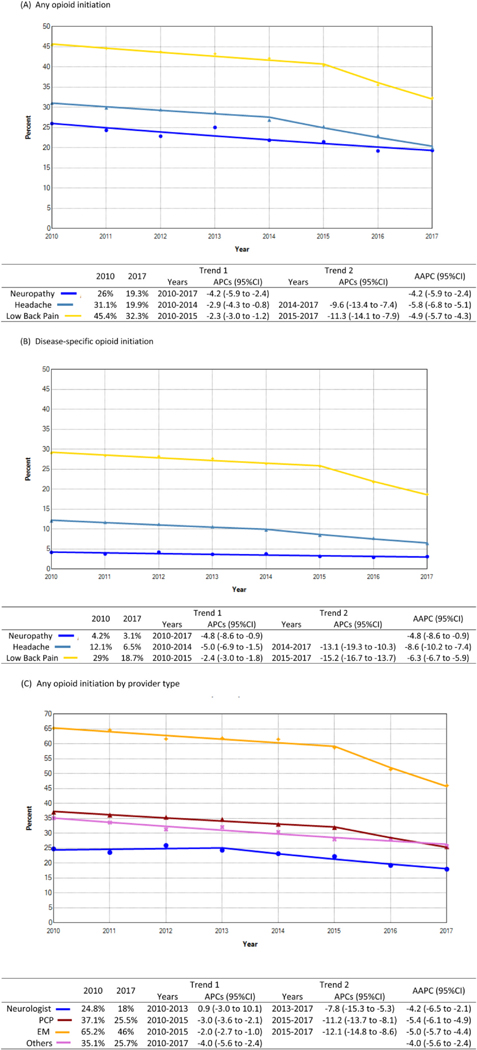
Neuropathy, headache, and low back pain (LBP) are common conditions requiring pain management. Yet little is known regarding whether access to specialists impacts opioid prescribing. We aimed to identify factors associated with opioid initiation among opioid-naïve older adults and evaluate how access to particular specialists impacts prescribing. This retrospective cohort study used a 20% Medicare sample from 2010 to 2017. Opioid initiation was defined as a first opioid prescription filled within 12 months after a diagnosis encounter. Disease-related opioid initiation was defined as a first opioid prescription filled within 7 days following a disease-specific claim. Logistic regression using generalized estimating equations was used to determine the association of patient demographics, provider types, and regional physician specialty density with disease-related opioid initiation, accounting for within-region correlation. We found opioid initiation steadily declined from 2010 to 2017 (neuropathy: 26-19%, headache: 31-20%, LBP: 45-32%), as did disease-related opioid initiation (4-3%, 12-7%, 29-19%) and 5 to 10% of initial disease-related prescriptions resulted in chronic opioid use within 12 months of initiation. Certain specialist visits were associated with a lower likelihood of disease-related opioid initiation compared with primary care. Residence in high neurologist density regions had a lower likelihood of disease-related opioid initiation (headache odds ratio [OR] .76 [95% CI: .63-.92]) and LBP (OR .7 [95% CI: .61-.81]) and high podiatrist density regions for neuropathy (OR .56 [95% CI: .41-.78]). We found that specialist visits and greater access to specialists were associated with a lower likelihood of disease-related opioid initiation. These data could inform strategies to perpetuate reductions in opioid use for these common pain conditions. PERSPECTIVE: This article presents how opioid initiation for opioid-naïve patients with newly diagnosed neuropathy, headache, and LBP varies across providers. Greater access to certain specialists decreased the likelihood of opioid initiation. Future work may consider interventions to support alternative treatments and better access to specialists in low-density regions.
神经病、头痛和下腰痛(LBP)是需要疼痛管理的常见病症。然而,对于专家的可及性是否会影响阿片类药物的处方,人们知之甚少。我们的目的是确定与阿片类药物初治老年患者开始使用阿片类药物相关的因素,并评估特定专家的可及性如何影响处方。这项回顾性队列研究使用了 2010 年至 2017 年的 Medicare 20%抽样数据。阿片类药物的初始使用被定义为在诊断性就诊后 12 个月内首次开具阿片类药物处方。与疾病相关的阿片类药物初始使用被定义为在特定疾病索赔后 7 天内首次开具阿片类药物处方。使用广义估计方程的逻辑回归用于确定患者人口统计学、提供者类型和区域医生专业密度与疾病相关阿片类药物初始使用的关联,同时考虑到区域内相关性。我们发现,从 2010 年到 2017 年,阿片类药物的初始使用稳步下降(神经病:26%-19%,头痛:31%-20%,LBP:45%-32%),与疾病相关的阿片类药物初始使用也同样下降(4%-3%,12%-7%,29%-19%),并且在初始疾病相关处方的 5%至 10%会导致在起始后 12 个月内慢性阿片类药物的使用。与初级保健相比,某些专科就诊与较低的疾病相关阿片类药物初始使用可能性相关。居住在神经科医生密度较高的地区与较低的疾病相关阿片类药物初始使用可能性相关(头痛的比值比[OR].76 [95%CI:.63-.92])和 LBP(OR.7 [95%CI:.61-.81])以及神经病高足病医生密度区域(OR.56 [95%CI:.41-.78])。我们发现,专科就诊和更多的专家可及性与较低的疾病相关阿片类药物初始使用可能性相关。这些数据可以为延续这些常见疼痛疾病的阿片类药物使用减少提供策略。观点:本文介绍了阿片类药物初治患者新诊断的神经病、头痛和 LBP 之间的阿片类药物初始使用情况在提供者之间的差异。更多地获得某些专科医生的治疗会降低开始使用阿片类药物的可能性。未来的研究可能需要考虑干预措施,以支持替代治疗方法,并改善在低密度地区获得专科医生的机会。