Chen Zhehan, Yu Jiayu, Cao Jiasheng, Lin Chenping, Hu Jiahao, Zhang Bin, Shen Jiliang, Feng Xu, Topatana Win, Chen Mingyu, Fang Haixing
The Second Clinical Medical College, Zhejiang Chinese Medical University, Hangzhou, Zhejiang, China.
Department of General Surgery, Sir Run-Run Shaw Hospital, Zhejiang University, Hangzhou, Zhejiang, China.
Front Oncol. 2023 Jul 4;13:1186378. doi: 10.3389/fonc.2023.1186378. eCollection 2023.
Although guidelines recommend extended cholecystectomy for T2 gallbladder cancer (GBC), the optimal hepatectomy strategy remains controversial. The study aims to compare the prognosis of T2 GBC patients who underwent wedge resection (WR) versus segment IVb and V resection (SR) of the liver.
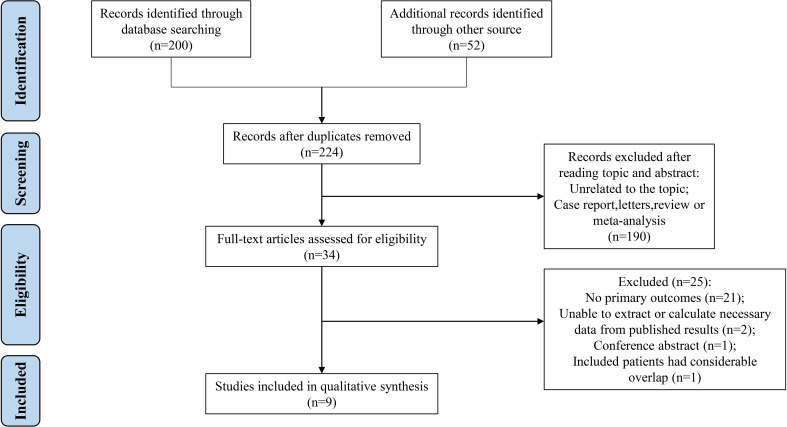
A specific search of online databases was performed from May 2001 to February 2023. The postoperative efficacy outcomes were synthesized and meta-analyses were conducted.
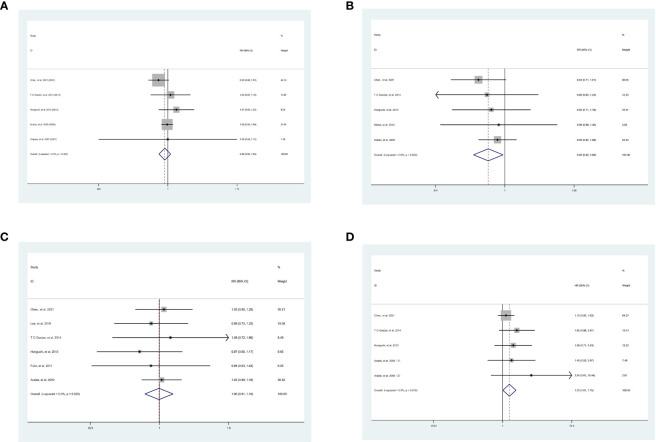
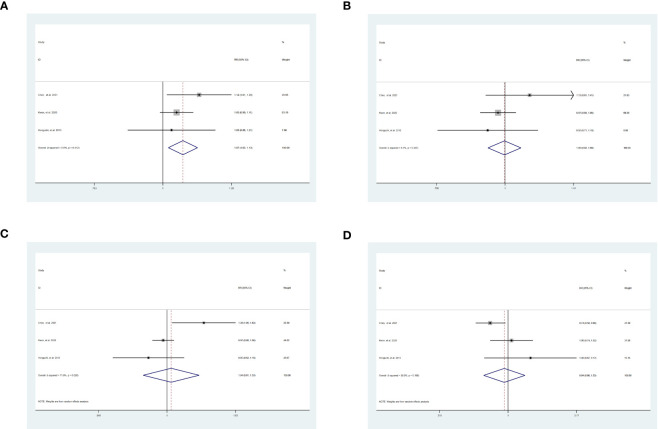
A total of 9 studies involving 2,086 (SR = 627, WR = 1,459) patients were included in the study. The primary outcomes included disease-free survival (DFS) and overall survival (OS). For DFS, the 1-year DFS was statistically higher in patients undergoing SR than WR [risk ratio (RR) = 1.07, 95% confidence interval (CI) = 1.02-1.13, = 0.007]. The 3-year DFS ( = 0.95), 5-year DFS ( = 0.77), and hazard ratio (HR) of DFS ( = 0.72) were similar between the two groups. However, the 3-year OS was significantly lower in patients who underwent SR than WR [RR = 0.90, 95% CI = 0.82-0.99, = 0.03]. Moreover, SR had a higher hazard HR of OS [HR = 1.33, 95% CI = 1.01-1.75, = 0.04]. No significant difference was found in 1-year ( = 0.32) and 5-year ( = 0.9) OS. For secondary outcomes, patients who received SR tended to develop postoperative complications (POC) [RR = 1.90, 95% CI = 1.00-3.60, = 0.05]. In addition, no significant differences in intrahepatic recurrence ( = 0.12) were observed.
In conclusion, SR can improve the prognosis of T2 GBC patients in DFS. In contrast to WR, the high HR and complications associated with SR cannot be neglected. Therefore, surgeons should evaluate the condition of the patients and take their surgical skills into account when selecting SR.
https://www.crd.york.ac.uk/prospero/, identifier, CRD42022362974.
尽管指南推荐对T2期胆囊癌(GBC)行扩大胆囊切除术,但最佳肝切除策略仍存在争议。本研究旨在比较接受楔形切除术(WR)与肝IVb和V段切除术(SR)的T2期GBC患者的预后。
于2001年5月至2023年2月对在线数据库进行了专项检索。综合术后疗效结果并进行荟萃分析。
本研究共纳入9项研究,涉及2086例患者(SR组 = 627例,WR组 = 1459例)。主要结局包括无病生存期(DFS)和总生存期(OS)。对于DFS,接受SR的患者1年DFS在统计学上高于接受WR的患者[风险比(RR) = 1.07,95%置信区间(CI) = 1.02 - 1.13,P = 0.007]。两组之间3年DFS(P = 0.95)、5年DFS(P = 0.77)和DFS的风险比(HR)(P = 0.72)相似。然而,接受SR的患者3年OS显著低于接受WR的患者[RR = 0.90,95% CI = 0.82 - 0.99,P = 0.03]。此外,SR组OS的HR更高[HR = 1.33,95% CI = 1.01 - 1.75,P = 0.04]。1年(P = 0.32)和5年(P = 可忽略)OS未发现显著差异。对于次要结局,接受SR的患者术后并发症(POC)发生率更高[RR = 1.90,95% CI = 1.00 - 3.60,P = 0.05]。此外,肝内复发未见显著差异(P = 0.12)。
总之,SR可改善T2期GBC患者的DFS预后。与WR相比,SR相关的高HR和并发症不容忽视。因此,外科医生在选择SR时应评估患者情况并考虑自身手术技能。