Pavlidis Efstathios T, Galanis Ioannis N, Pavlidis Theodoros E
2 Propedeutic Department of Surgery, Hippokration General Hospital, School of Medicine, Aristotle University of Thessaloniki, Thessaloniki 54642, Greece.
World J Gastrointest Oncol. 2024 Jan 15;16(1):13-29. doi: 10.4251/wjgo.v16.i1.13.
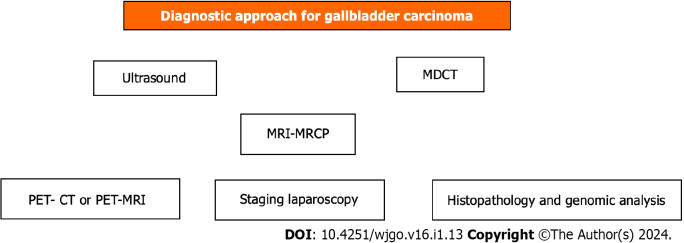
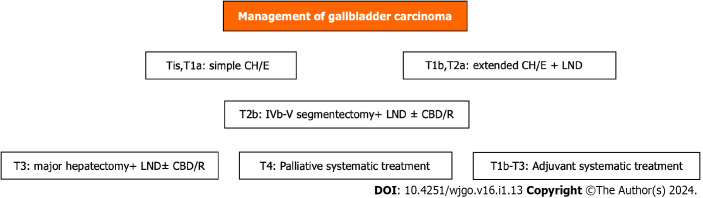
Gallbladder (GB) carcinoma, although relatively rare, is the most common biliary tree cholangiocarcinoma with aggressiveness and poor prognosis. It is closely associated with cholelithiasis and long-standing large (> 3 cm) gallstones in up to 90% of cases. The other main predisposing factors for GB carcinoma include molecular factors such as mutated genes, GB wall calcification (porcelain) or mainly mucosal microcalcifications, and GB polyps ≥ 1 cm in size. Diagnosis is made by ultrasound, computed tomography (CT), and, more precisely, magnetic resonance imaging (MRI). Preoperative staging is of great importance in decision-making regarding therapeutic management. Preoperative staging is based on MRI findings, the leading technique for liver metastasis imaging, enhanced three-phase CT angiography, or magnetic resonance angiography for major vessel assessment. It is also necessary to use positron emission tomography (PET)-CT or F-FDG PET-MRI to more accurately detect metastases and any other occult deposits with active metabolic uptake. Staging laparoscopy may detect dissemination not otherwise found in 20%-28.6% of cases. Multimodality treatment is needed, including surgical resection, targeted therapy by biological agents according to molecular testing gene mapping, chemotherapy, radiation therapy, and immunotherapy. It is of great importance to understand the updated guidelines and current treatment options. The extent of surgical intervention depends on the disease stage, ranging from simple cholecystectomy (T1a) to extended resections and including extended cholecystectomy (T1b), with wide lymph node resection in every case or IV-V segmentectomy (T2), hepatic trisegmentectomy or major hepatectomy accompanied by hepaticojejunostomy Roux-Y, and adjacent organ resection if necessary (T3). Laparoscopic or robotic surgery shows fewer postoperative complications and equivalent oncological outcomes when compared to open surgery, but much attention must be paid to avoiding injuries. In addition to surgery, novel targeted treatment along with immunotherapy and recent improvements in radiotherapy and chemotherapy (neoadjuvant-adjuvant capecitabine, cisplatin, gemcitabine) have yielded promising results even in inoperable cases calling for palliation (T4). Thus, individualized treatment must be applied.
胆囊癌虽然相对少见,但却是最常见的胆管癌,具有侵袭性且预后较差。在高达90%的病例中,它与胆石症及长期存在的大(>3厘米)胆结石密切相关。胆囊癌的其他主要诱发因素包括分子因素,如基因突变、胆囊壁钙化(瓷化)或主要是黏膜微钙化,以及直径≥1厘米的胆囊息肉。诊断通过超声、计算机断层扫描(CT),更准确的是磁共振成像(MRI)进行。术前分期对于治疗管理的决策至关重要。术前分期基于MRI检查结果(肝脏转移成像的主要技术)、增强三期CT血管造影或用于主要血管评估的磁共振血管造影。还需要使用正电子发射断层扫描(PET)-CT或F-FDG PET-MRI来更准确地检测转移灶和任何其他有活跃代谢摄取的隐匿性病灶。分期腹腔镜检查在20%-28.6%的病例中可能检测到其他方法未发现的播散情况。需要多模式治疗,包括手术切除、根据分子检测基因图谱使用生物制剂进行靶向治疗、化疗、放疗和免疫治疗。了解最新指南和当前治疗选择非常重要。手术干预的范围取决于疾病阶段,从单纯胆囊切除术(T1a)到扩大切除术,包括扩大胆囊切除术(T1b),每种情况都要进行广泛的淋巴结清扫或IV-V段切除术(T2)、肝三段切除术或伴有Roux-Y肝空肠吻合术的大肝切除术,必要时进行邻近器官切除术(T3)。与开放手术相比,腹腔镜或机器人手术术后并发症更少,肿瘤学结局相当,但必须非常注意避免损伤。除了手术,新型靶向治疗以及免疫治疗,以及放疗和化疗(新辅助-辅助卡培他滨、顺铂、吉西他滨)的最新进展,即使在需要姑息治疗的不可切除病例(T4)中也取得了有希望的结果。因此,必须采用个体化治疗。