Gao Xiaoyun, Chen Moxi, Liu Penghao, Zhou Shenyuan, Kong Sai, Zhang Junfeng, Cao Jun
Department of Anesthesiology, Shanghai Sixth People's Hospital, Shanghai, 200233, People's Republic of China.
J Pain Res. 2023 Jul 13;16:2375-2382. doi: 10.2147/JPR.S409721. eCollection 2023.
A novel ultrasound-guided paravertebral block, the edge laminar block (ELB) was reported recently. However, it was unclear how effective ELB was in comparison with traditional blocking methods. We conducted a trial to compare the analgesic efficacy of ELB with the thoracic paravertebral block (TPVB) and the retrolaminar block (RLB) in patients undergoing video-assisted thoracic surgery (VATS).
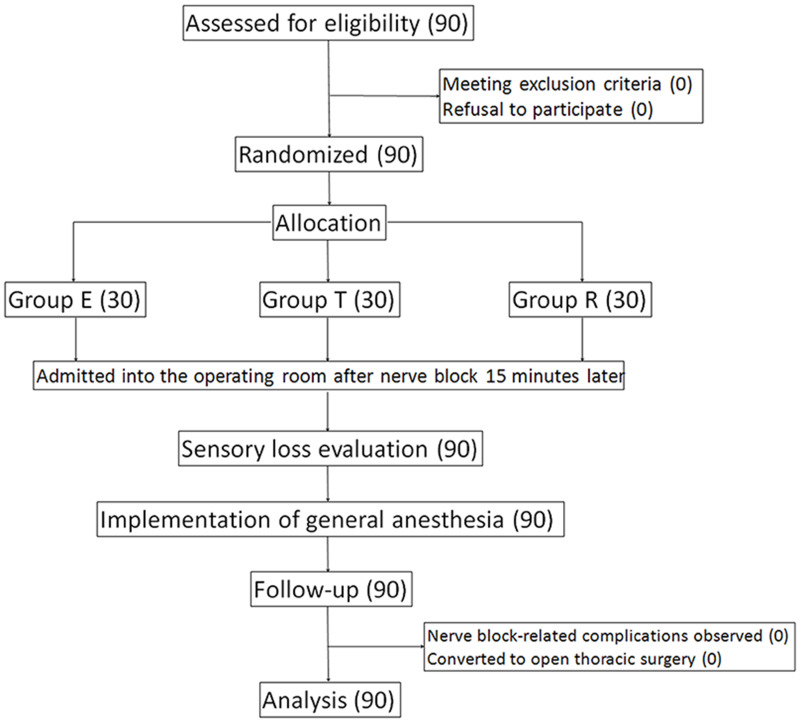
We identified 90 patients who were scheduled for VATS and randomly assigned them to three groups: ELB group (Group E), TPVB group (Group T), and RLB group (Group R). Each group underwent ELB, TPVB, and RLB, respectively, under ultrasound guidance before general anesthesia induction. All patients received post-operative routine analgesia protocol. Our primary outcome was the extent of dermatomal sensory loss on the midclavicular, midaxillary, and scapular lines, measured using a pinprick 15 minutes after the nerve block. Secondary outcomes included the intraoperative dose of sufentanil, the numerical rating scale (NRS) scores assessed in the post-anesthesia care unit (PACU) and at 6, 12, and 24 hours post-operatively, and pethidine administrated as analgesic rescue dose.
The percentages of nerve block range reaching the midclavicular line, midaxillary line, and scapular line in Group E were 96.7%, 93.3%, 93.3%, and 60% in Group T and 30%, 56.7%, and 96.7% in Group R, respectively. Group E had wider dermatomal sensory loss on the midclavicular line and midaxillary line compared to Group R ( 0.001) and had a wider range compared to Group T on the scapular line ( < 0.001). There was no significant difference in the intraoperative use of sufentanil in the three groups. Post-operative NRS scores at each time point were significantly lower in Group E than those in the other two groups ( < 0.01).
ELB had a wider nerve block range and applied better post-operative analgesia in comparison with TPVB and RLB.
最近报道了一种新型超声引导下的椎旁阻滞——边缘层流阻滞(ELB)。然而,与传统阻滞方法相比,ELB的效果如何尚不清楚。我们进行了一项试验,比较ELB与胸椎旁阻滞(TPVB)和椎板后阻滞(RLB)在电视辅助胸腔镜手术(VATS)患者中的镇痛效果。
我们确定了90例计划进行VATS的患者,并将他们随机分为三组:ELB组(E组)、TPVB组(T组)和RLB组(R组)。每组在全身麻醉诱导前,于超声引导下分别接受ELB、TPVB和RLB。所有患者均接受术后常规镇痛方案。我们的主要结局是在神经阻滞后15分钟,使用针刺法测量锁骨中线、腋中线和肩胛线上皮节感觉丧失的范围。次要结局包括术中舒芬太尼的用量、在麻醉后恢复室(PACU)以及术后6、12和24小时评估的数字评分量表(NRS)评分,以及作为镇痛补救剂量使用的哌替啶。
E组神经阻滞范围到达锁骨中线、腋中线和肩胛线的百分比分别为96.7%、93.3%、93.3%,T组分别为60%,R组分别为30%、56.7%和96.7%。与R组相比,E组在锁骨中线和腋中线的皮节感觉丧失范围更宽(P<0.001),与T组相比,在肩胛线的范围更宽(P<0.001)。三组术中舒芬太尼的使用无显著差异。E组术后各时间点的NRS评分均显著低于其他两组(P<0.01)。
与TPVB和RLB相比,ELB具有更广泛的神经阻滞范围且术后镇痛效果更佳。