Medical School of Chinese PLA, Beijing, China.
Senior Department of Cardiology, The Sixth Medical Center, Chinese PLA General Hospital, #6 FuCheng Road, Haidian District, Beijing, China.
Cardiovasc Diabetol. 2023 Jul 26;22(1):186. doi: 10.1186/s12933-023-01901-9.
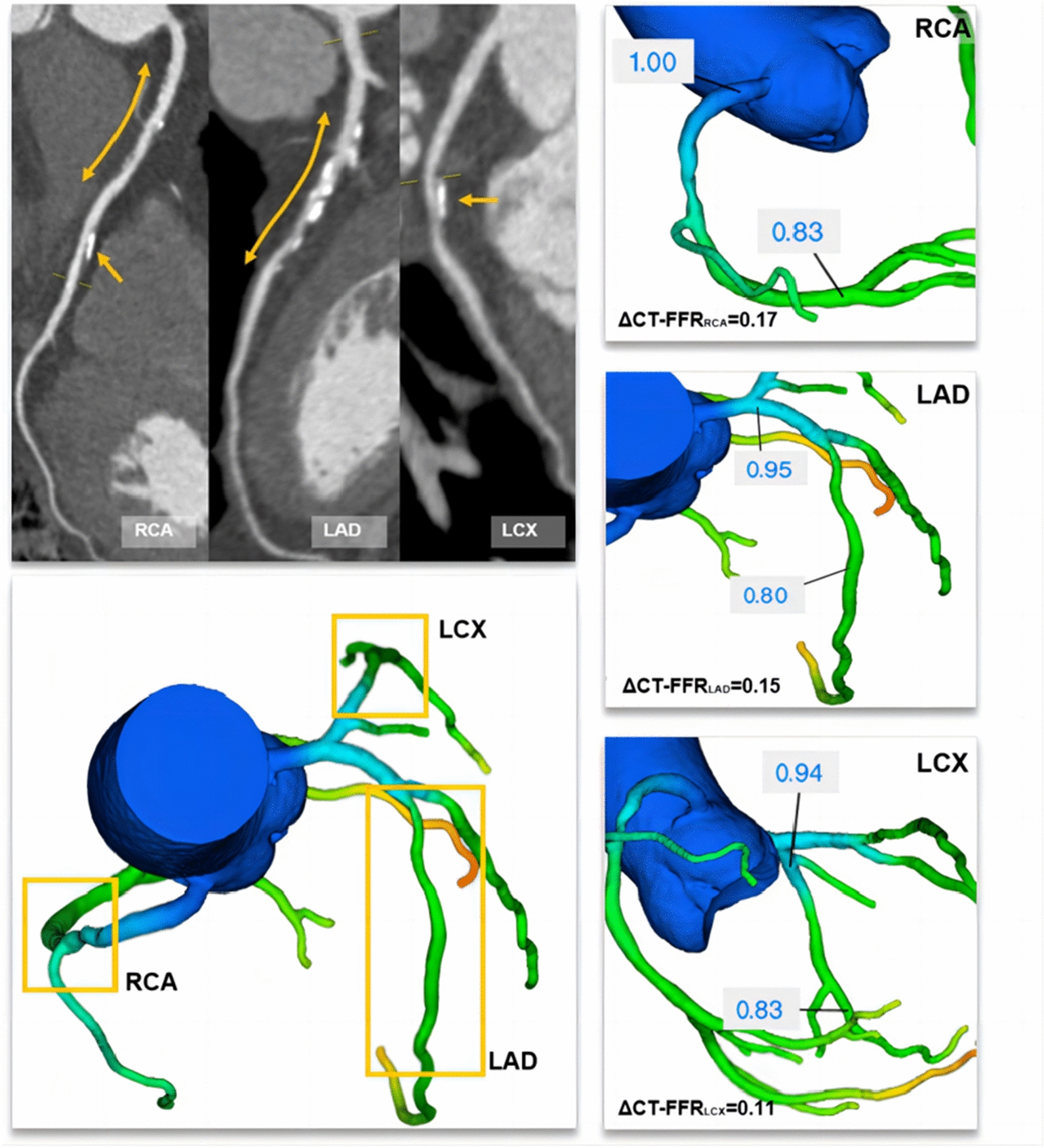
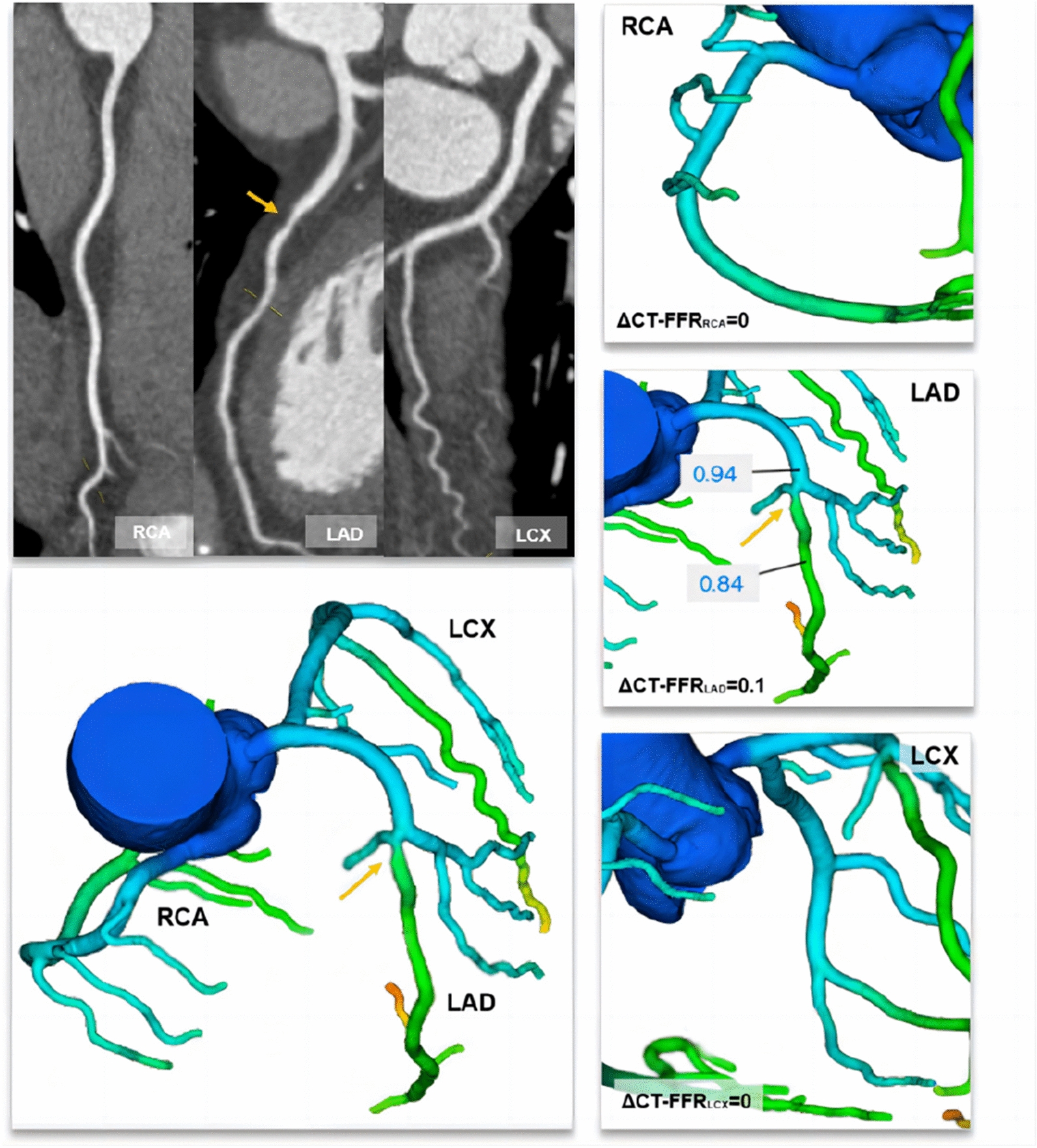
Coronary computed tomography angiography (CCTA)-derived fractional flow reserve (CT-FFR) enables physiological assessment and risk stratification, which is of significance in diabetic patients with nonobstructive coronary artery disease (CAD). We aim to evaluate prognostic value of the global trans-lesional CT-FFR gradient (GΔCT-FFR), a novel metric, in patients with diabetes without flow-limiting stenosis.
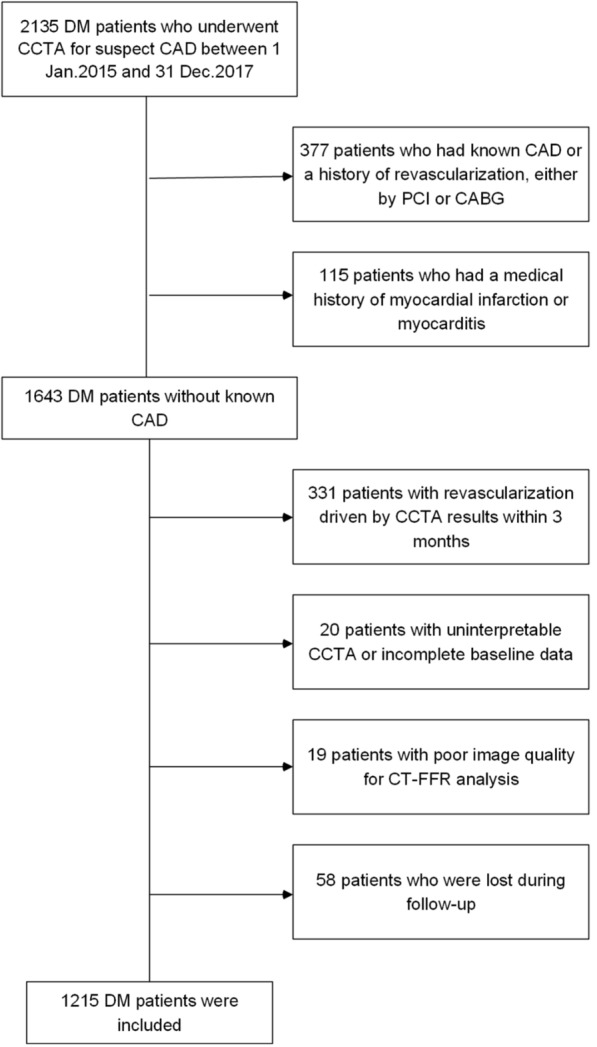
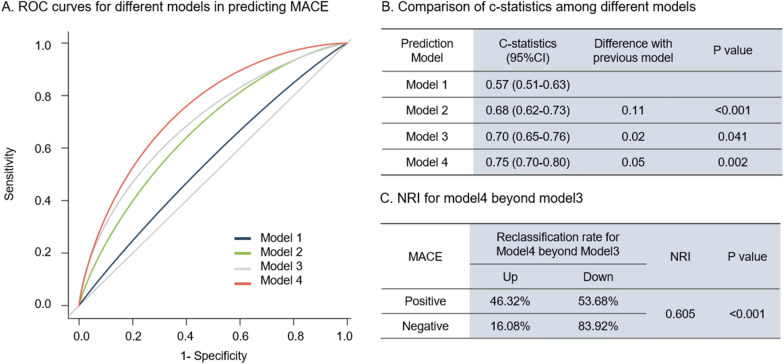
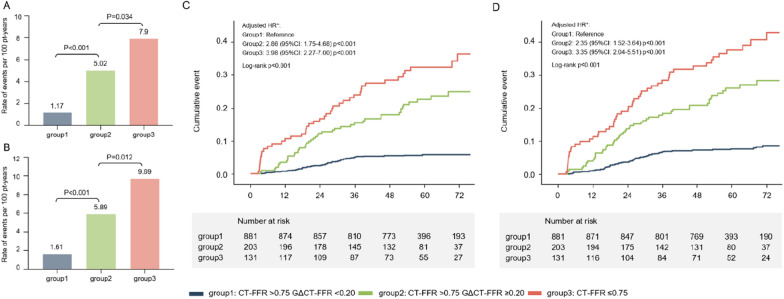
Patients with diabetes suspected of having CAD were prospectively enrolled. GΔCT-FFR was calculated as the sum of trans-lesional CT-FFR gradient in all epicardial vessels greater than 2 mm. Patients were stratified into low-gradient without flow-limiting group (CT-FFR > 0.75 and GΔCT-FFR < 0.20), high-gradient without flow-limiting group (CT-FFR > 0.75 and GΔCT-FFR ≥ 0.20), and flow-limiting group (CT-FFR ≤ 0.75). Discriminant ability for major adverse cardiovascular events (MACE) prediction was compared among 4 models [model 1: Framingham risk score; model 2: model 1 + Leiden score; model 3: model 2 + high-risk plaques (HRP); model 4: model 3 + GΔCT-FFR] to determine incremental prognostic value of GΔCT-FFR.
Of 1215 patients (60.1 ± 10.3 years, 53.7% male), 11.3% suffered from MACE after a median follow-up of 57.3 months. GΔCT-FFR (HR: 2.88, 95% CI 1.76-4.70, P < 0.001) remained independent risk factors of MACE in multivariable analysis. Compared with the low-gradient without flow-limiting group, the high-gradient without flow-limiting group (HR: 2.86, 95% CI 1.75-4.68, P < 0.001) was associated with higher risk of MACE. Among the 4 risk models, model 4, which included GΔCT-FFR, showed the highest C-statistics (C-statistics: 0.75, P = 0.002) as well as a significant net reclassification improvement (NRI) beyond model 3 (NRI: 0.605, P < 0.001).
In diabetic patients with non-obstructive CAD, GΔCT-FFR was associated with clinical outcomes at 5 year follow-up, which illuminates a novel and feasible approach to improved risk stratification for a global hemodynamic assessment of coronary artery in diabetic patients.
冠状动脉计算机断层血管造影术(CCTA)衍生的血流储备分数(CT-FFR)可实现生理学评估和风险分层,这对非阻塞性冠状动脉疾病(CAD)的糖尿病患者具有重要意义。我们旨在评估一种新的跨病变 CT-FFR 梯度(GΔCT-FFR)的预后价值,该指标在无血流限制狭窄的糖尿病患者中的应用。
前瞻性纳入疑似 CAD 的糖尿病患者。GΔCT-FFR 计算为所有大于 2mm 的心外膜血管的跨病变 CT-FFR 梯度之和。将患者分为低梯度无血流限制组(CT-FFR>0.75 且 GΔCT-FFR<0.20)、高梯度无血流限制组(CT-FFR>0.75 且 GΔCT-FFR≥0.20)和血流限制组(CT-FFR≤0.75)。比较 4 种模型[模型 1:弗莱明汉风险评分;模型 2:模型 1+莱顿评分;模型 3:模型 2+高危斑块(HRP);模型 4:模型 3+GΔCT-FFR]在预测主要不良心血管事件(MACE)方面的判别能力,以确定 GΔCT-FFR 的增量预后价值。
在 1215 例患者(60.1±10.3 岁,53.7%为男性)中,中位随访 57.3 个月后,有 11.3%的患者发生 MACE。多变量分析显示,GΔCT-FFR(HR:2.88,95%CI 1.76-4.70,P<0.001)仍是 MACE 的独立危险因素。与低梯度无血流限制组相比,高梯度无血流限制组(HR:2.86,95%CI 1.75-4.68,P<0.001)与 MACE 风险增加相关。在 4 种风险模型中,纳入 GΔCT-FFR 的模型 4 的 C 统计量(C 统计量:0.75,P=0.002)最高,与模型 3相比,显著提高了净重新分类改善(NRI)(NRI:0.605,P<0.001)。
在非阻塞性 CAD 的糖尿病患者中,GΔCT-FFR 与 5 年随访的临床结局相关,这为糖尿病患者冠状动脉的整体血流动力学评估提供了一种新的、可行的风险分层方法。