The Heller School for Social Policy & Management, Brandeis University, Waltham, MA, 02454-9110, USA.
Commonwealth Medicine, University of Massachusetts Medical School, Worcester, MA, USA.
BMC Health Serv Res. 2023 Jul 31;23(1):815. doi: 10.1186/s12913-023-09775-z.
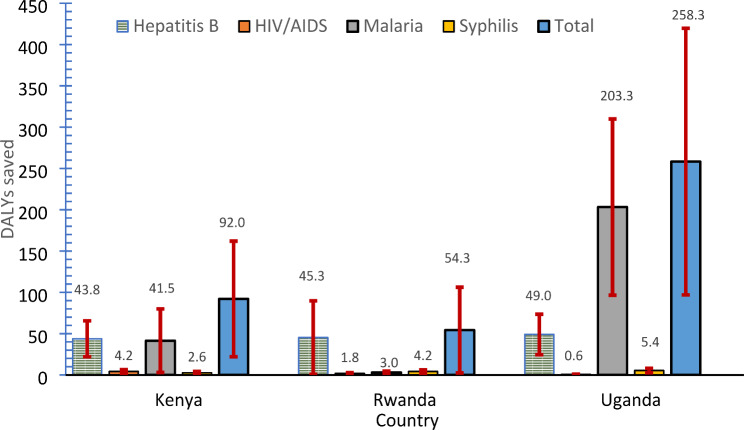
We performed an economic analysis of a new technology used in antenatal care (ANC) clinics, the ANC panel. Introduced in 2019-2020 in five Rwandan districts, the ANC panel screens for four infections [hepatitis B virus (HBV), human immunodeficiency virus (HIV), malaria, and syphilis] using blood from a single fingerstick. It increases the scope and sensitivity of screening over conventional testing.
We developed and applied an Excel-based economic and epidemiologic model to perform cost-effectiveness and cost-benefit analyses of this technology in Kenya, Rwanda, and Uganda. Costs include the ANC panel itself, its administration, and follow-up treatment. Effectiveness models predicted impacts on maternal and infant mortality and other outcomes. Key parameters are the baseline prevalence of each infection and the effectiveness of early treatment using observations from the Rwanda pilot, national and international literature, and expert opinion. For each parameter, we found the best estimate (with 95% confidence bound).
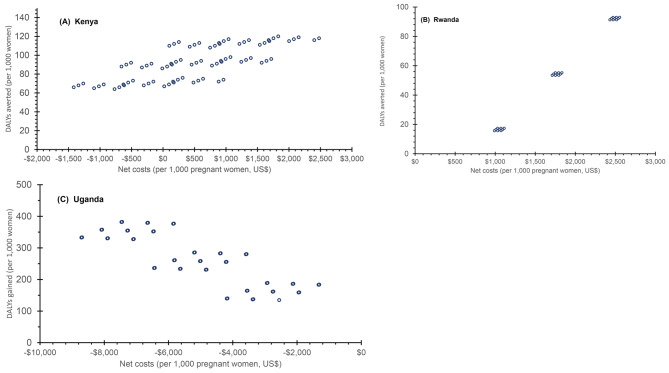
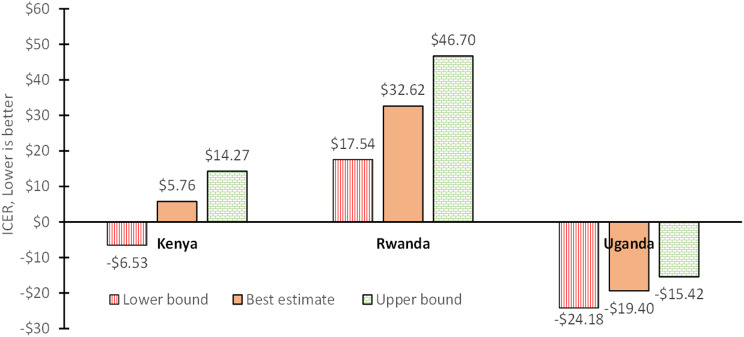
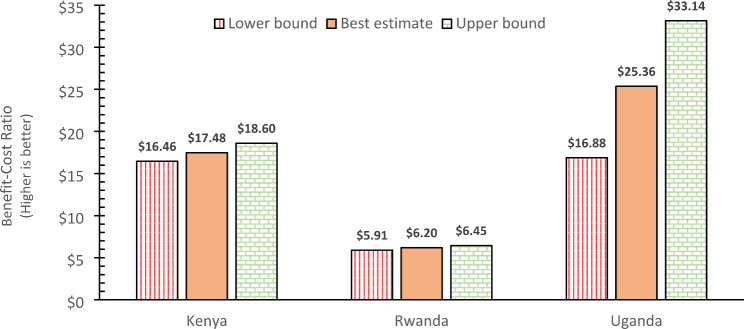
The ANC panel averted 92 (69-115) disability-adjusted life years (DALYs) per 1,000 pregnant women in ANC in Kenya, 54 (52-57) in Rwanda, and 258 (156-360) in Uganda. Net healthcare costs per woman ranged from $0.53 ($0.02-$4.21) in Kenya, $1.77 ($1.23-$5.60) in Rwanda, and negative $5.01 (-$6.45 to $0.48) in Uganda. Incremental cost-effectiveness ratios (ICERs) in dollars per DALY averted were $5.76 (-$3.50-$11.13) in Kenya, $32.62 ($17.54-$46.70) in Rwanda, and negative $19.40 (-$24.18 to -$15.42) in Uganda. Benefit-cost ratios were $17.48 ($15.90-$23.71) in Kenya, $6.20 ($5.91-$6.45) in Rwanda, and $25.36 ($16.88-$33.14) in Uganda. All results appear very favorable and cost-saving in Uganda.
Though subject to uncertainty, even our lowest estimates were still favorable. By combining field data and literature, the ANC model could be applied to other countries.
我们对产前护理(ANC)诊所使用的新技术(ANC 面板)进行了经济分析。该技术于 2019-2020 年在卢旺达的五个地区引入,使用单个手指刺血筛查四种感染[乙型肝炎病毒(HBV)、人类免疫缺陷病毒(HIV)、疟疾和梅毒]。它增加了筛查的范围和敏感性,超过了常规检测。
我们开发并应用了基于 Excel 的经济和流行病学模型,对肯尼亚、卢旺达和乌干达的这项技术进行了成本效益和成本效益分析。成本包括 ANC 面板本身、其管理和后续治疗。效果模型预测了对母婴死亡率和其他结果的影响。关键参数是每种感染的基线患病率以及使用卢旺达试点、国家和国际文献以及专家意见观察到的早期治疗效果。对于每个参数,我们都找到了最佳估计值(置信区间为 95%)。
ANC 面板在肯尼亚 ANC 中每 1000 名孕妇中避免了 92 个(69-115)残疾调整生命年(DALY),在卢旺达避免了 54 个(52-57),在乌干达避免了 258 个(156-360)。每位女性的净医疗保健成本从肯尼亚的 0.53 美元(0.02-4.21 美元)到卢旺达的 1.77 美元(1.23-5.60 美元)不等,而乌干达为负 5.01 美元(-6.45 美元至 0.48 美元)。肯尼亚每避免一个 DALY 的增量成本效益比(ICER)为 5.76 美元(-3.50-11.13 美元),卢旺达为 32.62 美元(17.54-46.70 美元),乌干达为负 19.40 美元(-24.18-15.42 美元)。肯尼亚的效益成本比为 17.48 美元(15.90-23.71 美元),卢旺达为 6.20 美元(5.91-6.45 美元),乌干达为 25.36 美元(16.88-33.14 美元)。所有结果在乌干达似乎都非常有利且具有成本效益。
即使我们的最低估计值仍存在不确定性,但仍具有优势。通过结合实地数据和文献,ANC 模型可以应用于其他国家。