Freytag Antje, Meissner Franziska, Krause Markus, Lehmann Thomas, Jansky Maximiliane Katharina, Marschall Ursula, Schmid Andreas, Schneider Nils, Vollmar Horst Christian, Wedding Ulrich, Ditscheid Bianka
Institut für Allgemeinmedizin, Universitätsklinikum Jena, Bachstr. 18, 07743, Jena, Deutschland.
Zentrum für Klinische Studien, Universitätsklinikum Jena, Jena, Deutschland.
Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2023 Oct;66(10):1135-1145. doi: 10.1007/s00103-023-03746-9. Epub 2023 Aug 3.
The main framework conditions for palliative care are set at the regional level. The scope of the forms of care used (outpatient, inpatient, general, specialized) varies widely. What is the quality of outcomes achieved by the palliative care provided on a federal states level? What are the associated costs of care?
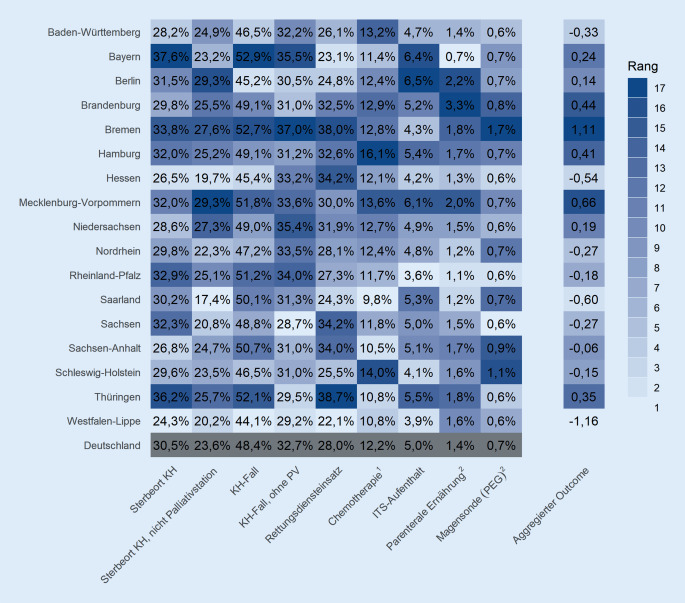
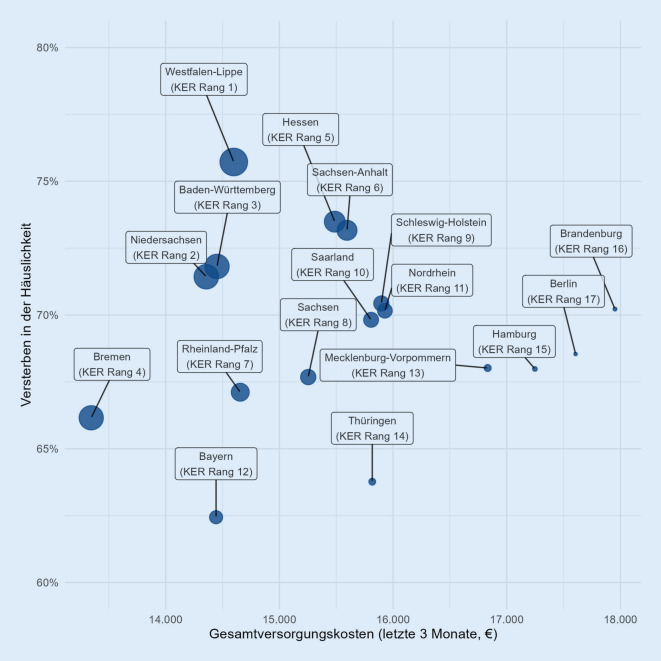
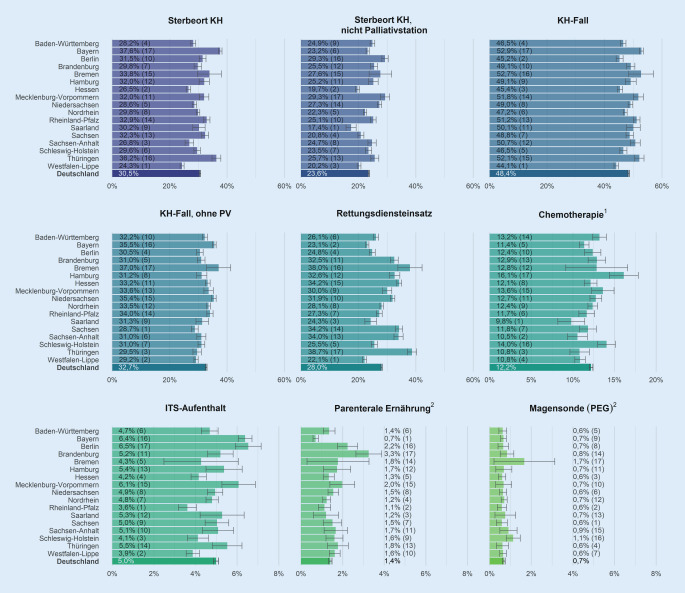
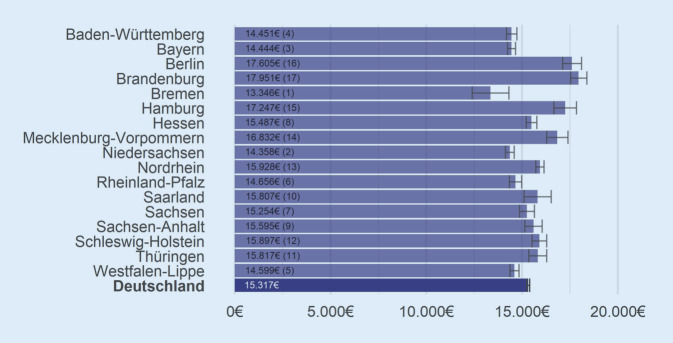
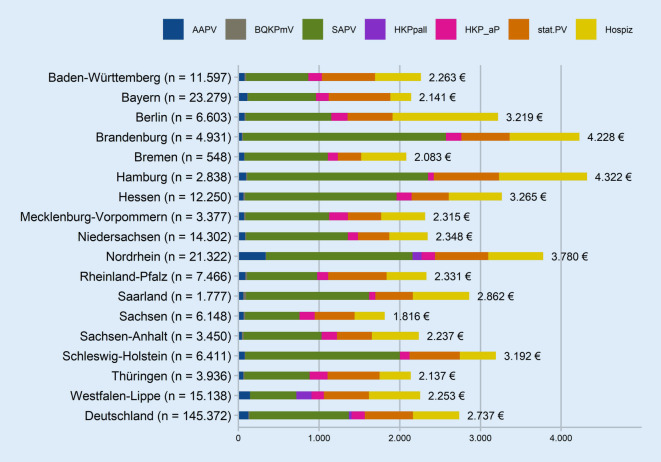
Retrospective observational study using BARMER claims data from 145,372 individuals who died between 2016 and 2019 and had palliative care in the last year of life. Regional comparison with regard to the following outcomes: proportion of palliative care patients who died in the hospital, potentially burdensome care in the last 30 days of life (ambulance calls, [intensive care] hospitalizations, chemotherapy, feeding tubes, parenteral nutrition), total cost of care (last three months), cost of palliative care (last year), and cost-effectiveness ratios. Calculation of patient/resident characteristic adjusted rates, costs, and ratios.
Federal states vary significantly with respect to the outcomes (also adjusted) of palliative care. Palliative care costs vary widely, most strongly for specialized outpatient palliative care (SAPV). Across all indicators and the cost-effectiveness ratio of total cost of care to at-home deaths, Westphalia-Lippe shows favorable results.
Regions with better quality and more favorable cost (ratios) can provide guidance for other regions. The extent to which the new federal SAPV agreement can incorporate the empirical findings should be reviewed. Patient-relevant outcome parameters should be given greater weight than parameters aiming at structures of care.
姑息治疗的主要框架条件在地区层面设定。所使用的护理形式(门诊、住院、普通、专科)范围差异很大。在联邦州层面提供的姑息治疗所取得的结果质量如何?相关的护理成本是多少?
采用回顾性观察研究,使用来自145372名在2016年至2019年间死亡且在生命最后一年接受姑息治疗的个体的BARMER理赔数据。就以下结果进行地区比较:在医院死亡的姑息治疗患者比例、生命最后30天潜在的繁重护理(救护车呼叫、[重症监护]住院、化疗、喂食管、肠外营养)、护理总成本(最后三个月)、姑息治疗成本(最后一年)以及成本效益比。计算患者/居民特征调整后的比率、成本和比例。
联邦州在姑息治疗的结果(经调整后)方面存在显著差异。姑息治疗成本差异很大,专科门诊姑息治疗(SAPV)的差异最为明显。在所有指标以及护理总成本与在家死亡的成本效益比方面,威斯特法伦 - 利珀表现出良好的结果。
质量更好且成本(比率)更有利的地区可为其他地区提供指导。应审查新的联邦SAPV协议能够纳入实证研究结果的程度。与患者相关的结果参数应比针对护理结构的参数更受重视。