Department of Surgery, Erasmus MC Cancer Institute, Rotterdam, The Netherlands.
Department of Surgery, Leiden University Medical Center, Leiden, The Netherlands.
BMC Cancer. 2023 Aug 7;23(1):728. doi: 10.1186/s12885-023-11141-5.
Surgical resection followed by adjuvant mFOLFIRINOX (5-fluorouracil with leucovorin, irinotecan, and oxaliplatin) is currently the standard of care for patients with resectable pancreatic cancer. The main concern regarding adjuvant chemotherapy is that only half of patients actually receive adjuvant treatment. Neoadjuvant chemotherapy, on the other hand, guarantees early systemic treatment and may increase chemotherapy use and thereby improve overall survival. Furthermore, it may prevent futile surgery in patients with rapidly progressive disease. However, some argue that neoadjuvant therapy delays surgery, which could lead to progression towards unresectable disease and thus offset the potential benefits. Comparison of perioperative (i.e., neoadjuvant and adjuvant) with (only) adjuvant administration of mFOLFIRINOX in a randomized controlled trial (RCT) is needed to determine the optimal approach.
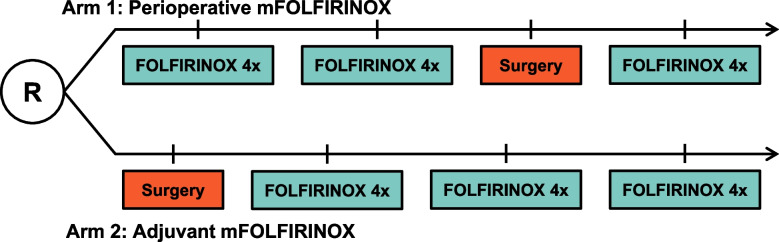
This multicenter, phase 3, RCT will include 378 patients with resectable pancreatic ductal adenocarcinoma with a WHO performance status of 0 or 1. Patients are recruited from 20 Dutch centers and three centers in Norway and Sweden. Resectable pancreatic cancer is defined as no arterial contact and ≤ 90 degrees venous contact. Patients in the intervention arm are scheduled for 8 cycles of neoadjuvant mFOLFIRINOX followed by surgery and 4 cycles of adjuvant mFOLFIRINOX (2-week cycle of oxaliplatin 85 mg/m, leucovorin 400 mg/m, irinotecan 150 mg/m at day 1, followed by 46 h continuous infusion of 5-fluorouracil 2400 g/m). Patients in the comparator arm start with surgery followed by 12 cycles of adjuvant mFOLFIRINOX. The primary outcome is overall survival by intention-to-treat. Secondary outcomes include progression-free survival, resection rate, quality of life, adverse events, and surgical complications. To detect a hazard ratio of 0.70 with 80% power, 252 events are needed. The number of events is expected to be reached after the inclusion of 378 patients in 36 months, with analysis planned 18 months after the last patient has been randomized.
The multicenter PREOPANC-3 trial compares perioperative mFOLFIRINOX with adjuvant mFOLFIRINOX in patients with resectable pancreatic cancer.
Clinical Trials: NCT04927780. Registered June 16, 2021.
手术切除联合辅助 mFOLFIRINOX(5-氟尿嘧啶+亚叶酸钙、伊立替康和奥沙利铂)是目前可切除胰腺癌患者的标准治疗方法。辅助化疗的主要问题是只有一半的患者实际接受了辅助治疗。新辅助化疗可保证早期全身性治疗,可能增加化疗的使用,从而提高总体生存率。此外,它还可以预防疾病快速进展的患者进行无效手术。然而,有人认为新辅助治疗会延迟手术,从而导致疾病向不可切除方向发展,从而抵消潜在的益处。需要通过随机对照试验(RCT)比较新辅助和辅助(仅辅助)mFOLFIRINOX 与(仅)辅助 mFOLFIRINOX 治疗可切除胰腺癌患者的疗效,以确定最佳治疗方法。
这项多中心、3 期 RCT 将纳入 378 例可切除胰腺导管腺癌患者,其世界卫生组织体力状态评分为 0 或 1。患者从 20 家荷兰中心和挪威、瑞典的 3 家中心招募。可切除的胰腺导管腺癌定义为没有动脉接触且静脉接触不超过 90 度。干预组的患者接受 8 个周期的新辅助 mFOLFIRINOX 治疗,随后进行手术,再接受 4 个周期的辅助 mFOLFIRINOX 治疗(2 周奥沙利铂 85mg/m、亚叶酸钙 400mg/m、伊立替康 150mg/m,第 1 天,随后氟尿嘧啶 2400g/m 持续输注 46 小时)。对照组的患者先进行手术,然后接受 12 个周期的辅助 mFOLFIRINOX 治疗。主要终点是意向治疗的总生存。次要结局包括无进展生存期、切除率、生活质量、不良事件和手术并发症。预计 36 个月内纳入 378 例患者可检测到 252 例事件,达到 80%的效力,计划在最后一例患者随机分组后 18 个月进行分析。
多中心 PREOPANC-3 试验比较了新辅助 mFOLFIRINOX 与可切除胰腺癌患者的辅助 mFOLFIRINOX。
临床试验:NCT04927780。于 2021 年 6 月 16 日注册。