Cirocchi Roberto, Amato Lavinia, Ungania Serena, Buononato Massimo, Tebala Giovanni Domenico, Cirillo Bruno, Avenia Stefano, Cozza Valerio, Costa Gianluca, Davies Richard Justin, Sapienza Paolo, Coccolini Federico, Mingoli Andrea, Chiarugi Massimo, Brachini Gioia
Department of Medicine and Surgery, S. Maria Hospital, University of Perugia, 05100 Terni, Italy.
Department of General and Emergency Surgery, S. Maria della Stella Hospital, 05018 Orvieto, Italy.
J Clin Med. 2023 Jul 26;12(15):4903. doi: 10.3390/jcm12154903.
This systematic review aims to investigate whether percutaneous transhepatic gallbladder biliary drainage (PTGBD) is superior to emergency cholecystectomy (EC) as a definitive treatment in high-risk patients with acute cholecystitis (AC).
A systematic literature search was performed until December 2022 using the Scopus, Medline/PubMed and Web of Science databases.
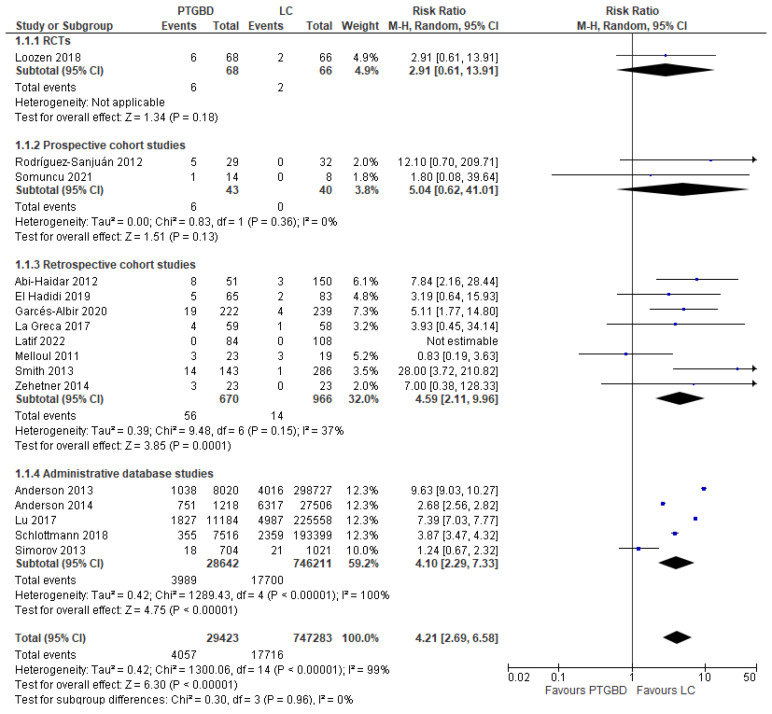
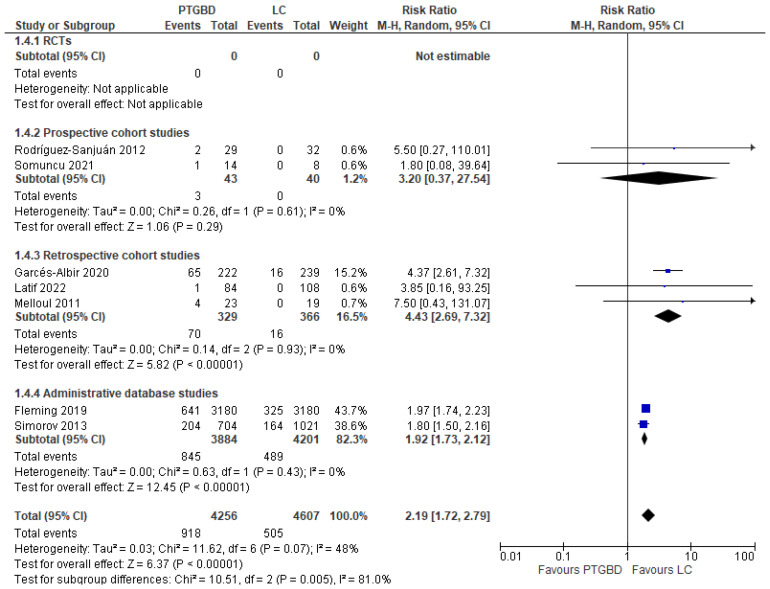
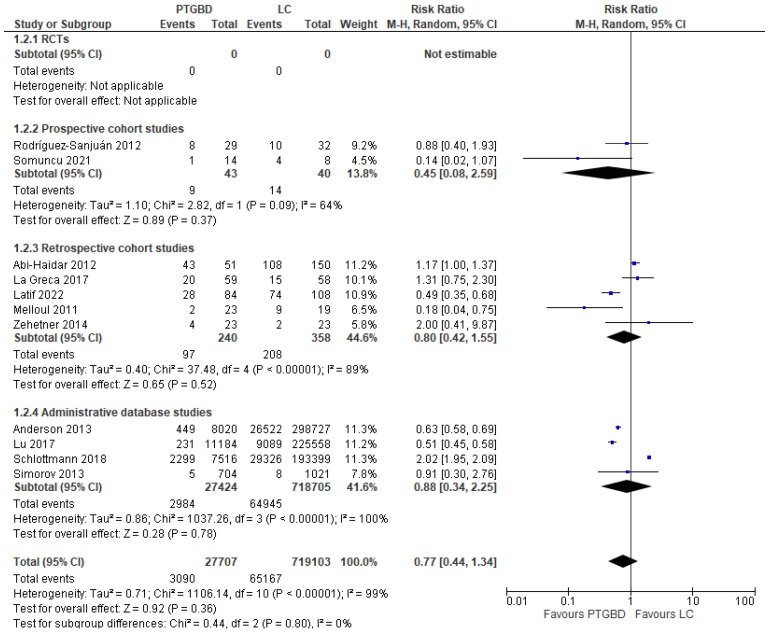
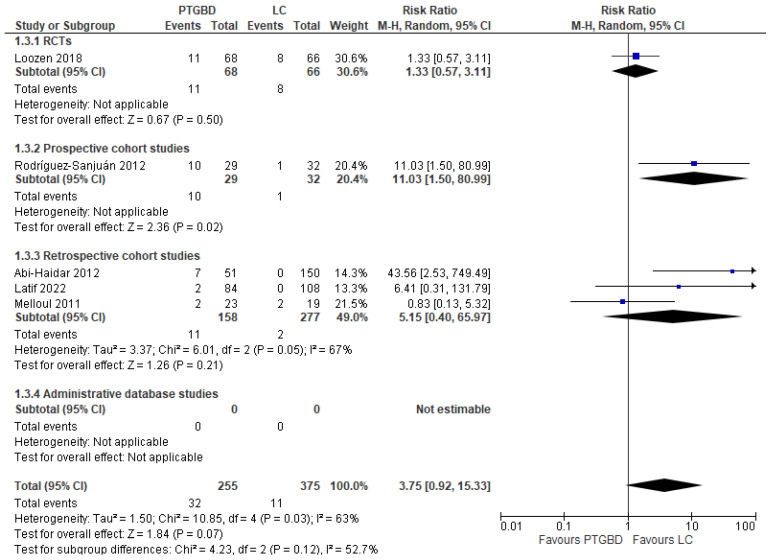
Seventeen studies have been included with a total of 783,672 patients (32,634 treated with PTGBD vs. 4663 who underwent laparoscopic cholecystectomy, 343 who had open cholecystectomy and 746,032 who had some form of cholecystectomy, but without laparoscopic or open approach being specified). An analysis of the results shows that PTGBD, despite being less invasive, is not associated with lower morbidity with respect to EC (RR 0.77 95% CI [0.44 to 1.34]; I = 99%; = 0.36). A lower postoperative mortality was reported in patients who underwent EC (2.37%) with respect to the PTGBD group (13.78%) (RR 4.21; 95% CI [2.69 to 6.58]; < 0.00001); furthermore, the risk of hospital readmission for biliary complications (RR 2.19 95% CI [1.72 to 2.79]; I = 48%; < 0.00001) and hospital stay (MD 4.29 95% CI [2.40 to 6.19]; < 0.00001) were lower in the EC group.
In our systematic review, the majority of studies have very low-quality evidence and more RCTs are needed; furthermore, PTGBD is inferior in the treatment of AC in high-risk patients. The definition of high-risk patients is important in interpreting the results, but the methods of assessment and definitions differ between studies. The results of our systematic review and meta-analysis failed to demonstrate any advantage of using PTGBD over ER as a definitive treatment of AC in critically ill patients, which suggests that EC should be considered as the treatment of choice even in very high-risk patients. Most likely, the inferiority of PTGBD versus early LC for high-risk patients is related to an association of various patient-side factor conditions and the severity of acute cholecystitis.
本系统评价旨在研究经皮经肝胆管胆囊引流术(PTGBD)作为高危急性胆囊炎(AC)患者的确定性治疗方法是否优于急诊胆囊切除术(EC)。
使用Scopus、Medline/PubMed和Web of Science数据库进行系统文献检索,直至2022年12月。
共纳入17项研究,总计783672例患者(32634例接受PTGBD治疗,4663例接受腹腔镜胆囊切除术,343例接受开腹胆囊切除术,746032例接受某种形式的胆囊切除术,但未明确说明是腹腔镜还是开腹手术)。结果分析表明,尽管PTGBD侵入性较小,但与EC相比,其发病率并无降低(风险比0.77,95%置信区间[0.44至1.34];I² = 99%;P = 0.36)。与PTGBD组(13.78%)相比,接受EC的患者术后死亡率较低(2.37%)(风险比4.21;95%置信区间[2.69至6.58];P < 0.00001);此外,EC组胆道并发症再次入院风险(风险比2.19,95%置信区间[1.72至2.79];I² = 48%;P < 0.00001)和住院时间(平均差4.29,95%置信区间[2.40至6.19];P < 0.00001)更低。
在我们的系统评价中,大多数研究证据质量极低,需要更多随机对照试验;此外,PTGBD在高危患者AC治疗中效果较差。高危患者的定义对解释结果很重要,但不同研究的评估方法和定义存在差异。我们的系统评价和荟萃分析结果未能证明在危重症患者中使用PTGBD作为AC确定性治疗方法优于急诊胆囊切除术,这表明即使在极高危患者中,也应将EC视为首选治疗方法。很可能,PTGBD相对于高危患者早期腹腔镜胆囊切除术的劣势与多种患者因素状况和急性胆囊炎的严重程度相关。