Serban Dragos, Socea Bogdan, Balasescu Simona Andreea, Badiu Cristinel Dumitru, Tudor Corneliu, Dascalu Ana Maria, Vancea Geta, Spataru Radu Iulian, Sabau Alexandru Dan, Sabau Dan, Tanasescu Ciprian
4th Department of Surgery, University Emergency Hospital Bucharest, 050098 Bucharest, Romania.
Faculty of Medicine, "Carol Davila" University of Medicine and Pharmacy, 020021 Bucharest, Romania.
Medicina (Kaunas). 2021 Mar 2;57(3):230. doi: 10.3390/medicina57030230.
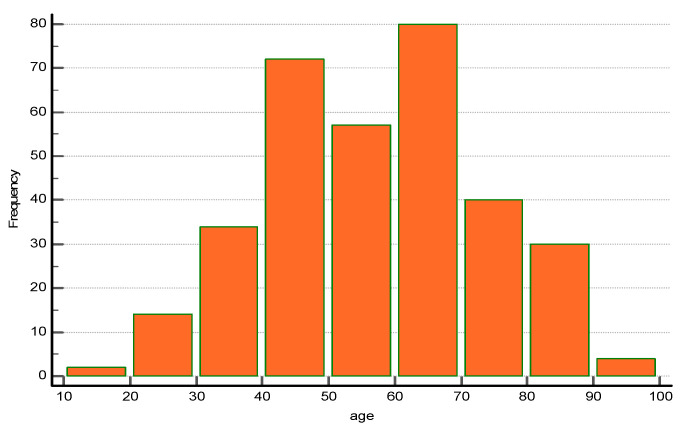
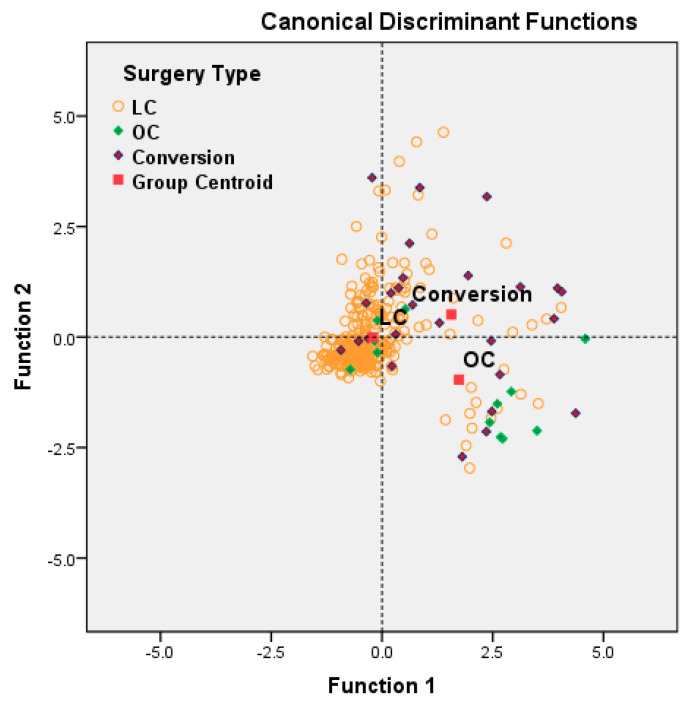
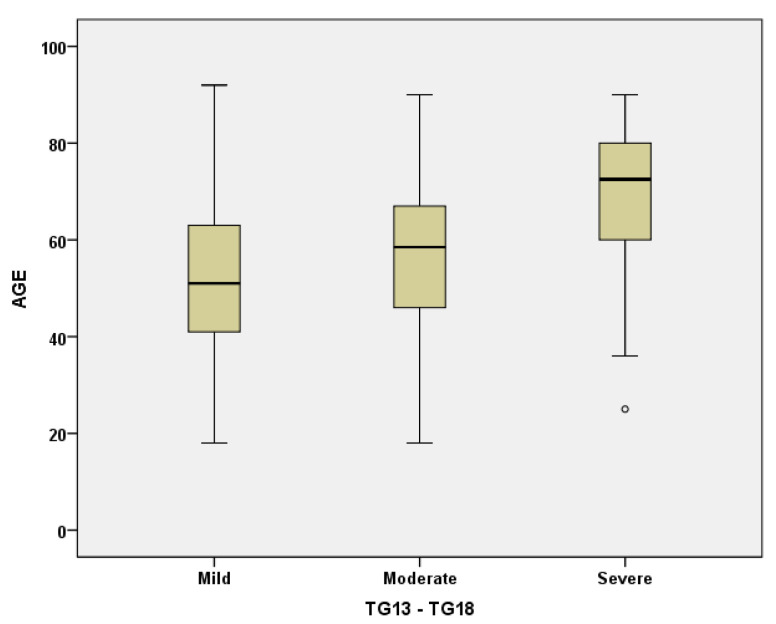
This study investigates the impact of age upon the safety and outcomes of laparoscopic cholecystectomy performed for acute cholecystitis, by a multivariate approach. A 2-year retrospective study was performed on 333 patients admitted for acute cholecystitis who underwent emergency cholecystectomy. The patients included in the study group were divided into four age subgroups: A ≤49 years; B: 50-64 years; C: 65-79 years; D ≥80 years. Surgery after 72 h from onset ( = 0.007), severe forms, and higher American Society of Anesthesiologists Physical Status Classification and Charlson comorbidity index scores ( < 0.001) are well correlated with older age. Both cardiovascular and surgical related complications were significantly higher in patients over 50 years ( = 0.045), which also proved to be a turning point for increasing the rate of conversion and open surgery. However, the comparative incidence did not differ significantly between patients aged from 50-64 years, 65-79 years and over 80 years (6.03%, 9.09% and 5.8%, respectively). Laparoscopic cholecystectomy (LC) was the most frequently used surgical approach in the treatment of acute cholecystitis in all age groups, with better outcomes than open cholecystectomy in terms of decreased overall and postoperative hospital stay, reduced surgery related complications, and the incidence of acute cardiovascular events in the early postoperative period ( < 0.001). The degree of systemic inflammation was the main factor that influenced the adverse outcome of LC in the elderly. Among comorbidities, diabetes was associated with increased surgical and systemic postoperative morbidity, while stroke and chronic renal insufficiency were correlated with a high risk of cardiovascular complications. With adequate perioperative care, the elderly has much to gain from the benefits of a minimally invasive approach, which allows a decreased rate of postoperative complications and a reduced hospital stay.
本研究采用多变量方法,调查年龄对急性胆囊炎行腹腔镜胆囊切除术的安全性和结局的影响。对333例因急性胆囊炎入院并接受急诊胆囊切除术的患者进行了一项为期2年的回顾性研究。研究组纳入的患者被分为四个年龄亚组:A组≤49岁;B组:50 - 64岁;C组:65 - 79岁;D组≥80岁。发病后72小时后手术(P = 0.007)、病情严重程度、较高的美国麻醉医师协会身体状况分类和查尔森合并症指数评分(P < 0.001)与年龄较大密切相关。50岁以上患者的心血管并发症和手术相关并发症均显著更高(P = 0.045),这也被证明是增加中转率和开放手术率的一个转折点。然而,50 - 64岁患者、65 - 79岁患者和超过80岁患者之间的相对发生率差异无统计学意义(分别为6.03%、9.09%和5.8%)。腹腔镜胆囊切除术(LC)是所有年龄组治疗急性胆囊炎最常用的手术方法,在降低总体住院时间和术后住院时间、减少手术相关并发症以及术后早期急性心血管事件发生率方面,其结局优于开放胆囊切除术(P < 0.001)。全身炎症程度是影响老年患者LC不良结局的主要因素。在合并症中,糖尿病与手术和全身术后发病率增加相关,而中风和慢性肾功能不全与心血管并发症的高风险相关。通过充分的围手术期护理,老年人可从微创方法的益处中获益良多,这可降低术后并发症发生率并缩短住院时间。