Lersch Robert, Mandilaras Guido, Schrader Meike, Anselmino Felicitas, Haas Nikolaus A, Jakob André
Department of Paediatric Cardiology and Paediatric Intensive Care, Ludwig-Maximillian-University Munich, Munich, Germany.
Department of Paediatrics, Clinic Starnberg, Starnberg, Germany.
Front Pediatr. 2023 Jul 28;11:1210940. doi: 10.3389/fped.2023.1210940. eCollection 2023.
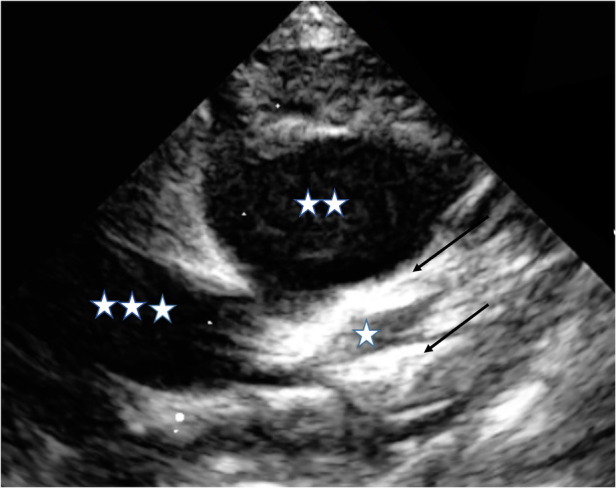
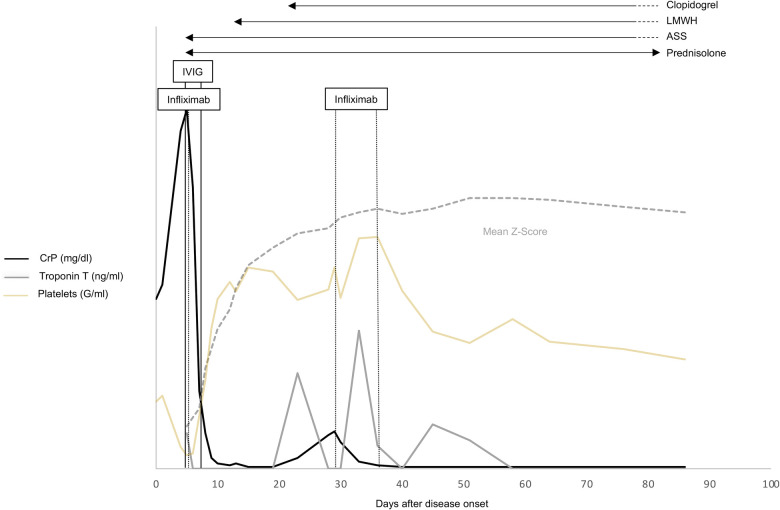
A small group of patients with Kawasaki disease (KD) demonstrates resistance to standard therapy, putting them at high risk for an unfavorable prognosis, especially regarding coronary artery aneurysms. Although adding corticosteroids to first-line i.v. immunoglobulins (IVIGs) is considered beneficial, and despite timely treatment initiation, very young infants, in particular, can present an unfavorable clinical course. We report on a 3-month-old boy with a clinically severe KD phenotype involving the early development of giant coronary artery aneurysms. Because of his poor response to the first course of IVIG and prednisolone, we administered infliximab. His clinical condition improved after that, and his temperature dropped. Inflammatory markers however did not recover completely, and he remained subfebrile. In addition, as the coronary artery dimensions deteriorated, a second IVIG course was administered and prednisolone continued at the initial dosage. Although fever and routine inflammatory parameters normalized, close follow-up investigations revealed both still increasing coronary artery dimensions and renewed rise in inflammatory parameters, necessitating two more infliximab administrations in addition to continuous prednisolone. Because of the coronary artery dimensions (left anterior descending artery, 4.9 mm, Z-score 11.1; right coronary artery 5.8 mm, Z-score 15.5), dual platelet inhibitory therapy with ASA and later clopidogrel combined with low-molecular heparin was indicated. Four weeks after his initial KD diagnosis, we detected no renewed increase in inflammatory markers; at that time, we observed a slight reduction in coronary dimensions. In summary, despite timely guideline-fulfilling therapy, the prolonged clinical course of this very young infant with KD entailing the development of giant coronary artery aneurysms makes us question whether this age group may benefit from early, even more intense therapy.
一小部分川崎病(KD)患者对标准治疗表现出耐药性,这使他们面临不良预后的高风险,尤其是在冠状动脉瘤方面。尽管在一线静脉注射免疫球蛋白(IVIG)中添加皮质类固醇被认为是有益的,而且尽管及时开始治疗,但特别是非常小的婴儿可能会出现不良的临床病程。我们报告了一名3个月大的男孩,其临床症状严重,患有KD,伴有巨大冠状动脉瘤的早期形成。由于他对第一疗程的IVIG和泼尼松龙反应不佳,我们给予了英夫利昔单抗。此后他的临床状况有所改善,体温下降。然而,炎症标志物并未完全恢复,他仍有低热。此外,随着冠状动脉尺寸恶化,给予了第二疗程的IVIG,并继续按初始剂量使用泼尼松龙。尽管发热和常规炎症参数恢复正常,但密切的随访调查显示冠状动脉尺寸仍在增加,炎症参数再次升高,因此除了持续使用泼尼松龙外,还需要再给予两次英夫利昔单抗。由于冠状动脉尺寸(左前降支动脉,4.9 mm,Z评分11.1;右冠状动脉5.8 mm,Z评分15.5),因此建议联合使用阿司匹林和氯吡格雷进行双重血小板抑制治疗,并联合低分子肝素。在他最初被诊断为KD四周后,我们未检测到炎症标志物再次升高;此时,我们观察到冠状动脉尺寸略有减小。总之,尽管及时进行了符合指南的治疗,但这名患有KD且伴有巨大冠状动脉瘤形成的非常小的婴儿的临床病程延长,这使我们质疑这个年龄组是否可能从早期、甚至更强化的治疗中获益。