Calabrese Cassandra, Atefi Gelareh, Evans Kristin A, Moynihan Meghan, Palmer Liisa, Wu Sze-Jung
Rheumatic & Immunologic Diseases, Cleveland Clinic, Cleveland, Ohio, USA.
US Medical, AstraZeneca Pharmaceuticals LP, Wilmington, Delaware, USA.
RMD Open. 2023 Aug;9(3). doi: 10.1136/rmdopen-2023-003250.
To identify risk factors for progression to severe COVID-19 and estimate the odds of severe COVID-19 associated with vaccination among patients with systemic lupus erythematosus (SLE).
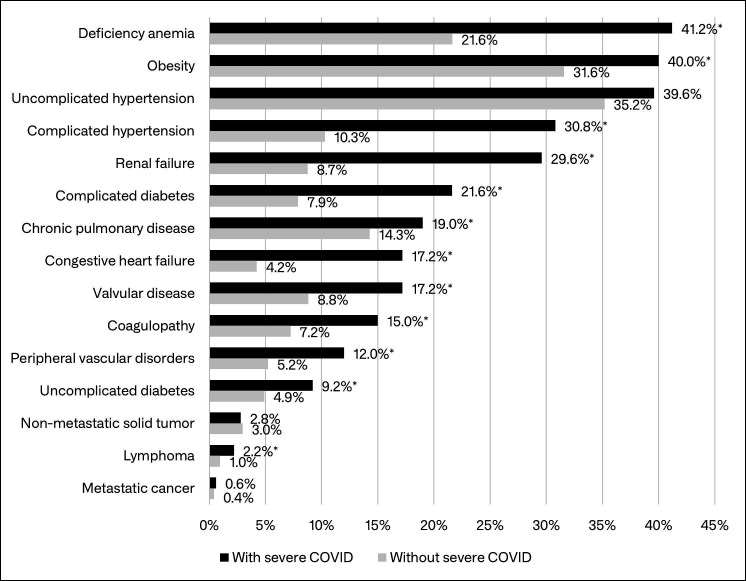
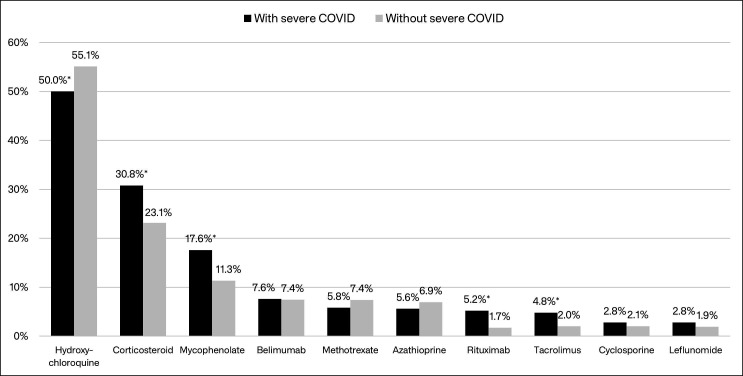
This retrospective cohort study identified adults with SLE in the Merative™ MarketScan Databases. Patients were continuously enrolled the year before 1 April 2020 (baseline) and had a COVID-19 diagnosis between 1 April 2020 and the earliest of death, enrolment end or 31 December 2021. Severe COVID-19 was defined as hospitalisation with a COVID-19 diagnosis. Demographics on 1 April 2020, baseline comorbidities, corticosteroid use ≤30 days before COVID-19 diagnosis and other SLE medication use ≤6 months before COVID-19 diagnosis were assessed. Vaccination was identified by claims for a COVID-19 vaccine or vaccine administration. Backward stepwise logistic regression estimated odds of progression to severe COVID-19 associated with patient characteristics and vaccination.
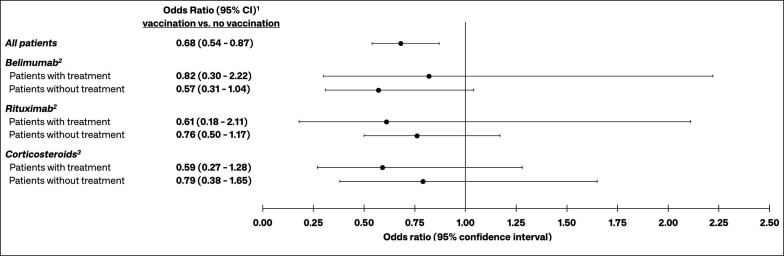
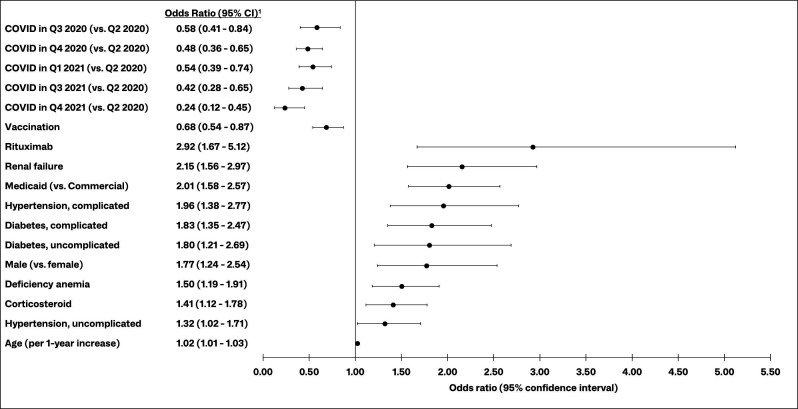
Among 2890 patients with SLE with COVID-19, 500 (16.4%) had a COVID-19-related hospitalisation. Significant risk factors for progression to severe COVID-19 included rituximab (OR (95% CI) 2.92 (1.67 to 5.12)), renal failure (2.15 (95% CI 1.56 to 2.97)), Medicaid (vs Commercial; 2.01 (95% CI 1.58 to 2.57)), complicated hypertension (1.96 (95% CI 1.38 to 2.77)) and time of infection, among others. Vaccination had a significant protective effect (0.68(95% CI 0.54 to 0.87)) among all patients with SLE with COVID-19, but the effect was not significant among those with prior use of belimumab, rituximab or corticosteroids.
Certain chronic comorbidities and SLE medications increase the odds of progression to severe COVID-19 among patients with SLE, but vaccination confers significant protection. Vaccine effectiveness may be attenuated by SLE treatments. Protective measures such as pre-exposure prophylaxis and booster vaccines should be encouraged among patients with SLE.
确定进展为重症新型冠状病毒肺炎(COVID-19)的危险因素,并估计系统性红斑狼疮(SLE)患者中与接种疫苗相关的重症COVID-19的几率。
这项回顾性队列研究在Merative™ MarketScan数据库中识别出患有SLE的成年人。患者在2020年4月1日之前的一年(基线)连续入组,并在2020年4月1日至最早的死亡、入组结束或2021年12月31日期间被诊断为COVID-19。重症COVID-19定义为因COVID-19诊断而住院。评估了2020年4月1日的人口统计学数据、基线合并症、COVID-19诊断前≤30天使用皮质类固醇以及COVID-19诊断前≤6个月使用其他SLE药物的情况。通过COVID-19疫苗或疫苗接种的报销记录来确定疫苗接种情况。向后逐步逻辑回归估计了与患者特征和疫苗接种相关的进展为重症COVID-19的几率。
在2890例患有COVID-19的SLE患者中,500例(16.4%)因COVID-19住院。进展为重症COVID-19的显著危险因素包括利妥昔单抗(比值比(OR)(95%置信区间)2.92(1.67至5.12))、肾衰竭(2.15(95%置信区间1.56至2.97))、医疗补助(与商业保险相比;2.01(95%置信区间1.58至2.57))、复杂性高血压(1.96(95%置信区间1.38至2.77))以及感染时间等。在所有患有COVID-19的SLE患者中,疫苗接种具有显著的保护作用(0.68(95%置信区间0.54至0.87)),但在先前使用贝利尤单抗、利妥昔单抗或皮质类固醇的患者中,这种作用不显著。
某些慢性合并症和SLE药物会增加SLE患者进展为重症COVID-19的几率,但疫苗接种可提供显著保护。SLE治疗可能会削弱疫苗的有效性。应鼓励SLE患者采取如暴露前预防和加强疫苗接种等保护措施。