Dhamija Gaurav, Kapoor Mudit, Kim Rockli, Subramanian S V
Indian Institute of Technology Hyderabad, Telangana, India.
Indian Statistical Institute, New Delhi, India.
SSM Popul Health. 2023 Aug 4;23:101482. doi: 10.1016/j.ssmph.2023.101482. eCollection 2023 Sep.
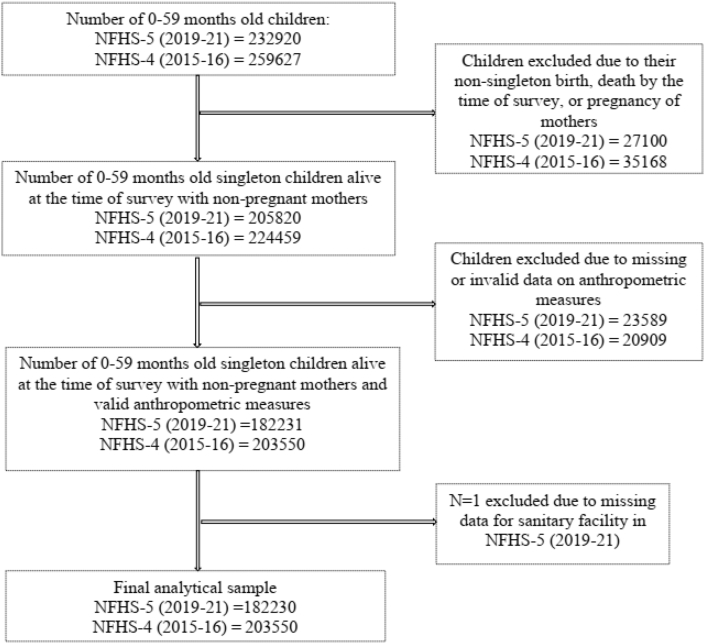
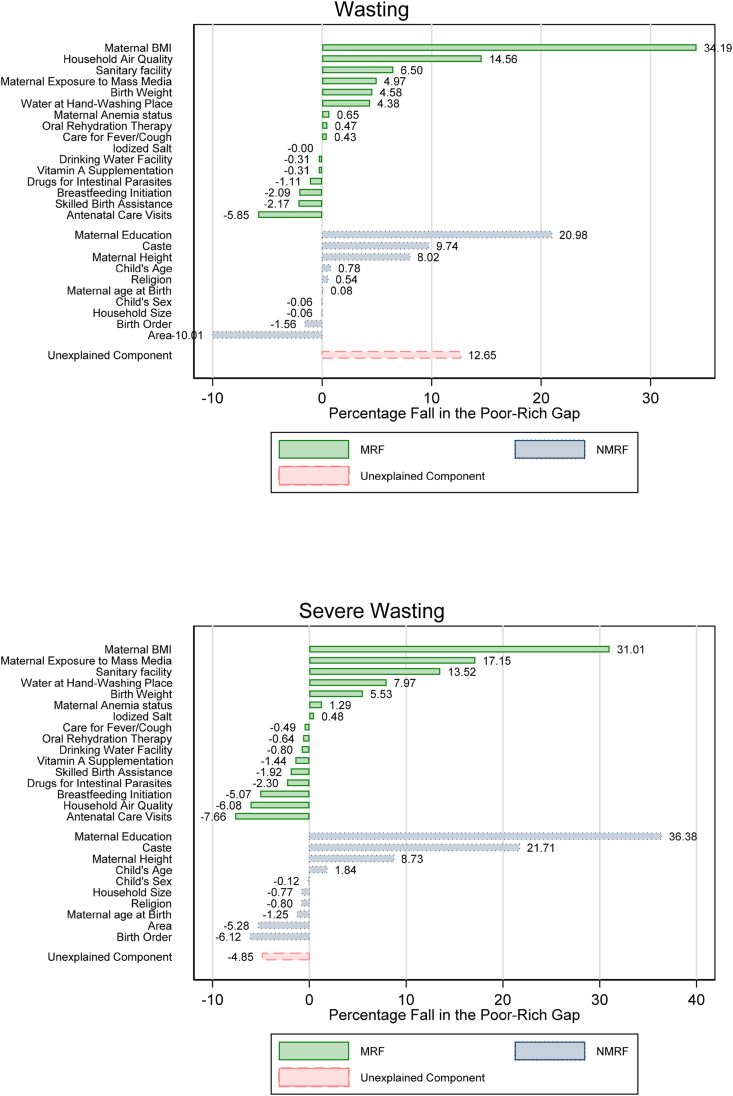
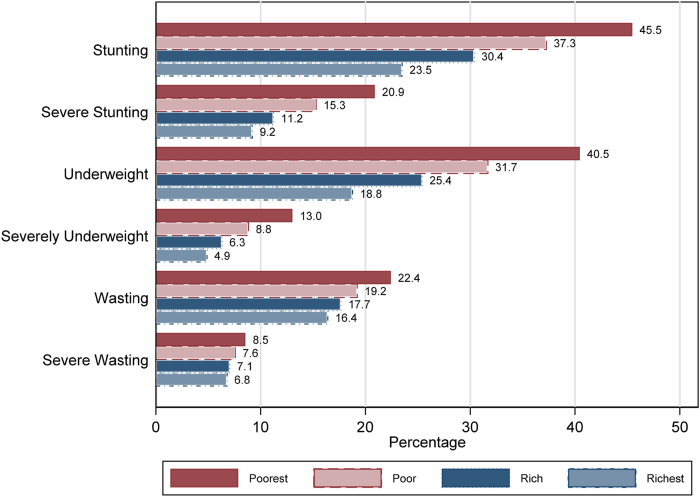
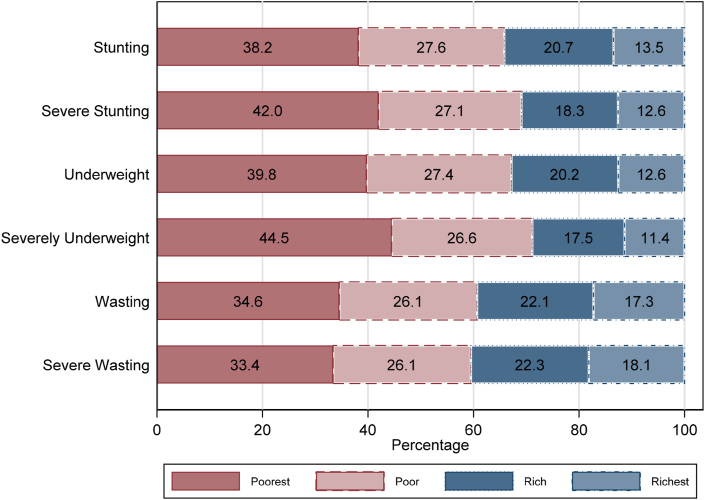
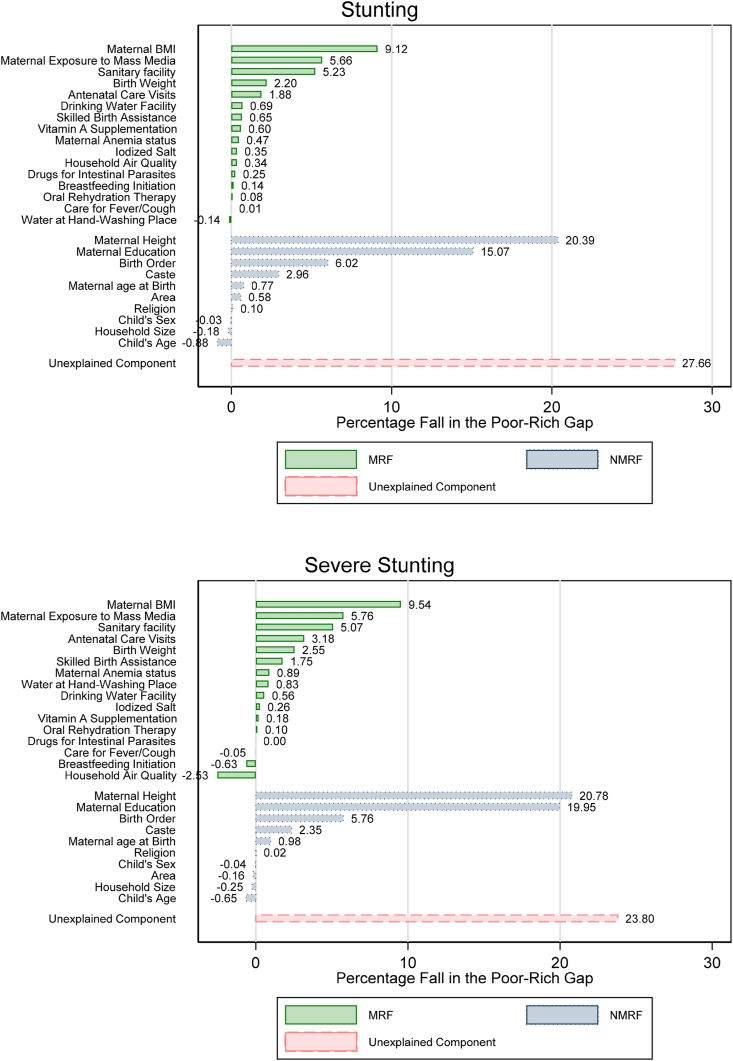
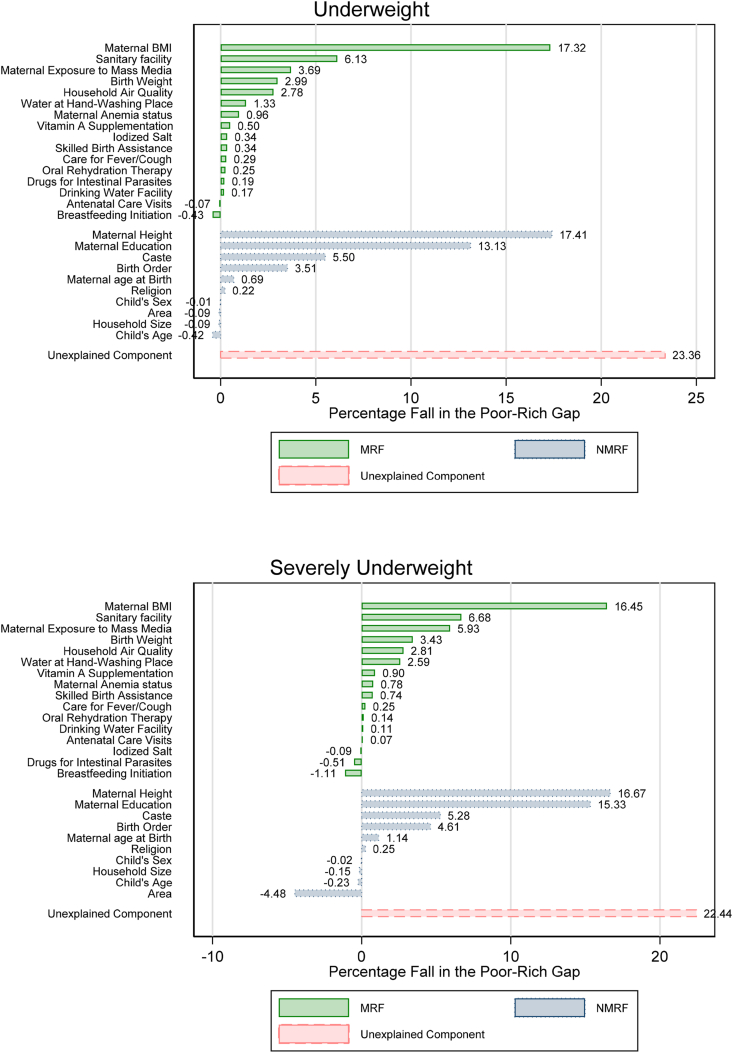
Wealth inequality in anthropometric failure is a persistent concern for policymakers in India. This necessitates a comprehensive analysis and identification of various risk factors that can explain the poor-rich gap in anthropometric failure among children in India. We analyze the fifth and fourth rounds of the Indian National Family Health Survey collected from June 2019 to April 2021 and January 2015 to December 2016, respectively. Two samples of children aged 0-59 and 6-23 months old with singleton birth, alive at the time of the survey with non-pregnant mothers, and with valid data on stunting, severe stunting, underweight, severely underweight, wasting, and severe wasting are included in the analytical samples from both rounds. We estimate the wealth gradients and distribution of wealth among children with anthropometric failure. Wealth gap in anthropometric failure is identified using logistic regression analysis. The contribution of risk factors in explaining the poor-rich gap in AF is estimated by the multivariate decomposition analysis. We observe a negative wealth gradient for each measure of anthropometric failure. Wealth distributions indicate that at least 60% of the population burden of anthropometric failure is among the poor and poorest wealth groups. Even among children with similar modifiable risk factors, children from poor and poorest backgrounds have a higher prevalence of anthropometric failure compared to children from the richest backgrounds. Maternal BMI, exposure to mass media, and access to sanitary facility are the most significant risk factors that explain the poor-rich gap in anthropometric failure. This evidence suggests that the burden of anthropometric failure and its risk factors are unevenly distributed in India. The policy interventions focusing on maternal and child health, implemented with a targeted approach prioritizing the vulnerable groups, can only partially bridge the poor-rich gap in anthropometric failure. The role of anti-poverty programs and growth is essential to narrow this gap in anthropometric failure.
印度人体测量指标不达标的财富不平等问题一直是政策制定者关注的焦点。这就需要对各种风险因素进行全面分析和识别,以解释印度儿童在人体测量指标不达标的贫富差距。我们分别分析了2019年6月至2021年4月以及2015年1月至2016年12月收集的印度全国家庭健康调查的第五轮和第四轮数据。分析样本包括两轮调查中年龄在0 - 59个月和6 - 23个月的单胎出生儿童,调查时母亲未怀孕且存活,并有发育迟缓、严重发育迟缓、体重不足、严重体重不足、消瘦和严重消瘦的有效数据。我们估计了人体测量指标不达标的儿童的财富梯度和财富分布。通过逻辑回归分析确定人体测量指标不达标的财富差距。通过多变量分解分析估计风险因素在解释人体测量指标不达标的贫富差距中的作用。我们观察到,在人体测量指标不达标的各项指标中都存在负财富梯度。财富分布表明,至少60%的人体测量指标不达标的人口负担集中在贫困和最贫困的财富群体中。即使在具有相似可改变风险因素的儿童中,来自贫困和最贫困背景的儿童相比最富有背景的儿童,人体测量指标不达标的患病率更高。母亲的体重指数、接触大众媒体以及获得卫生设施是解释人体测量指标不达标的贫富差距的最重要风险因素。这一证据表明,印度人体测量指标不达标的负担及其风险因素分布不均。以弱势群体为优先目标实施的母婴健康政策干预措施,只能部分弥合人体测量指标不达标的贫富差距。反贫困计划和经济增长对于缩小人体测量指标不达标的差距至关重要。