Department of Heart Failure and Transplantation, Inova Heart and Vascular Institute, Falls Church, VA (J.F.G., C.R.d., P.S.).
Department of Pediatrics, Inova L.J. Murphy Children's Hospital, Falls Church, VA (J.F.G.).
Circulation. 2023 Aug 22;148(8):679-694. doi: 10.1161/CIRCULATIONAHA.123.062847. Epub 2023 Aug 21.
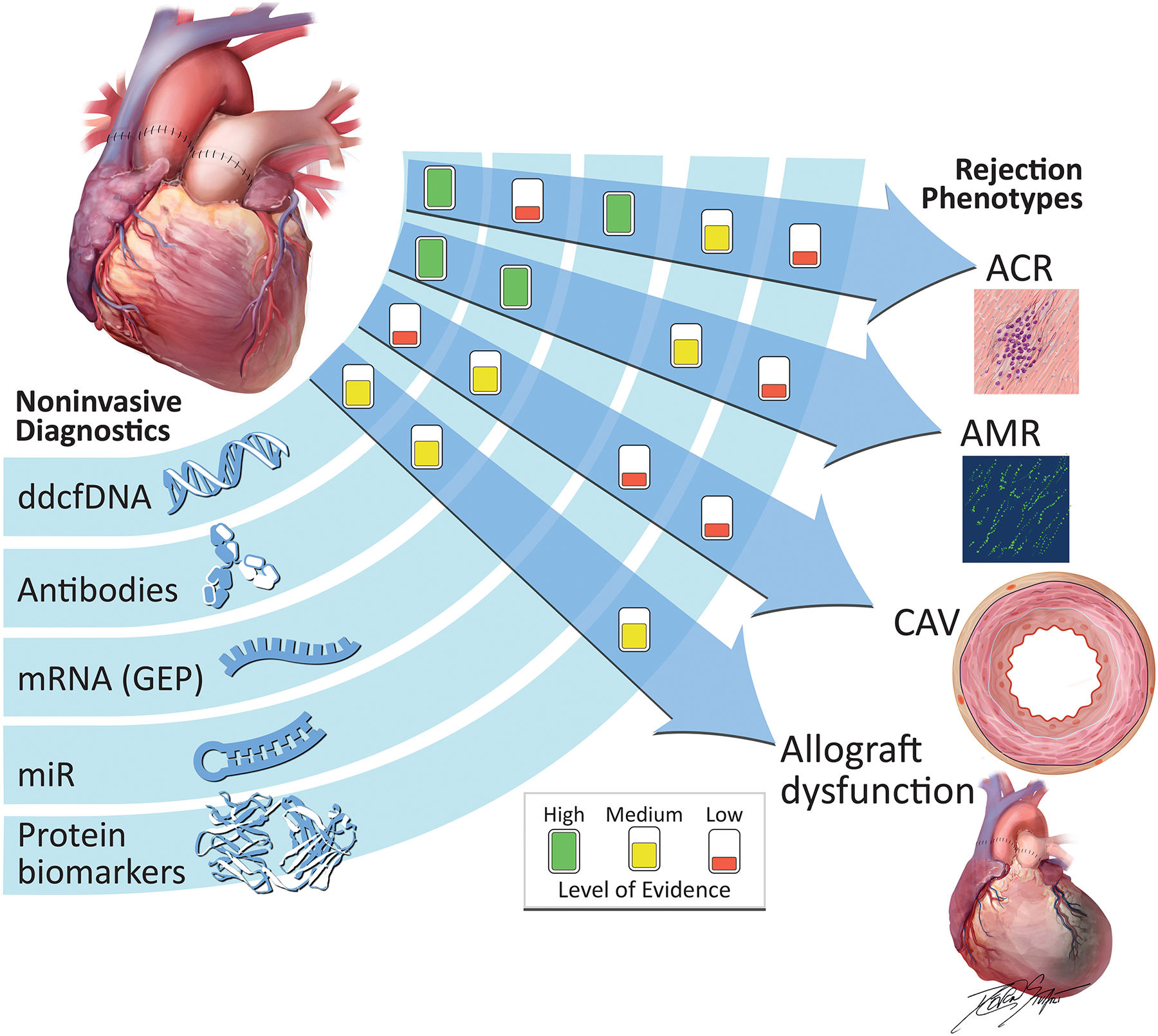
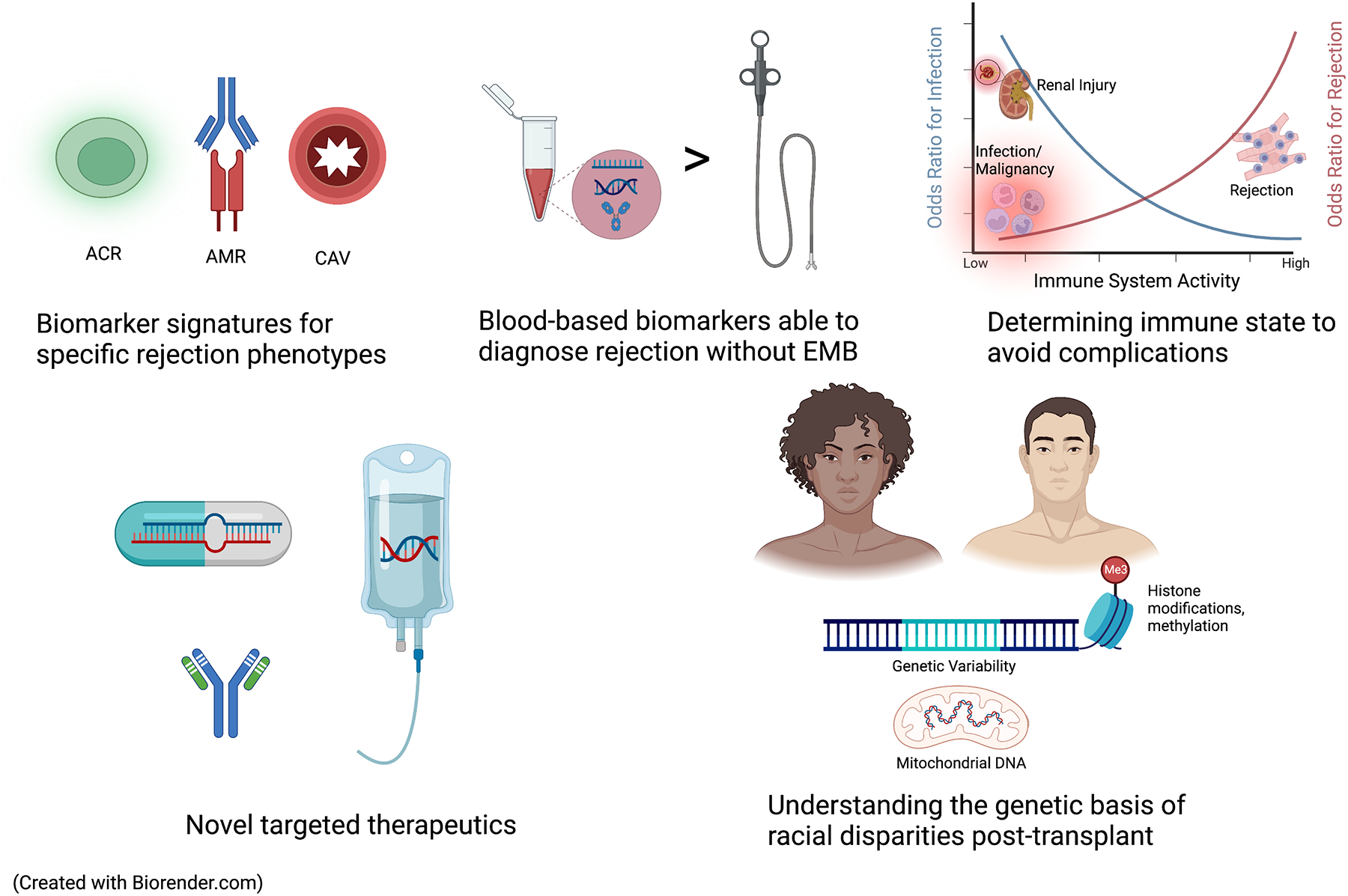
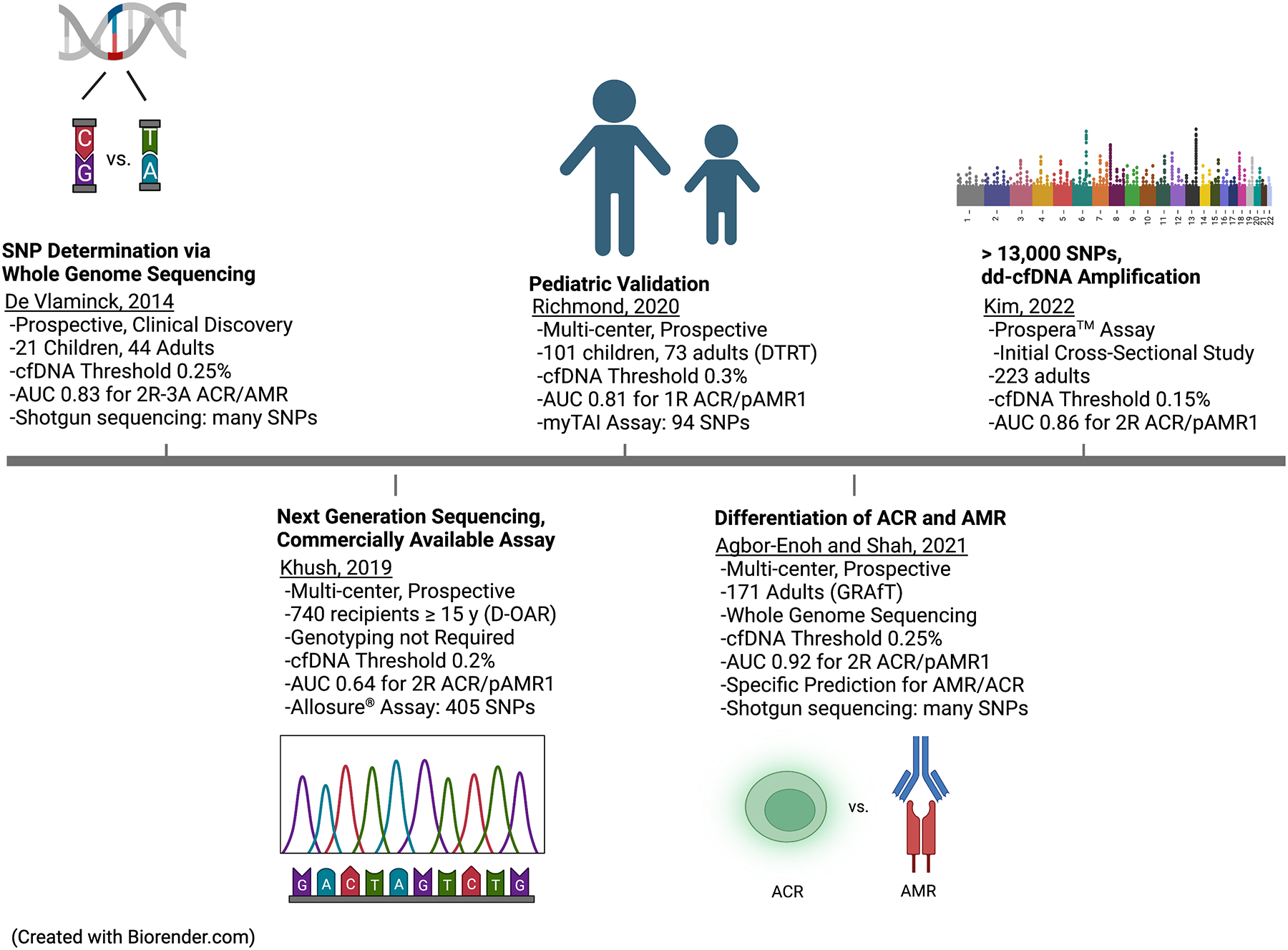
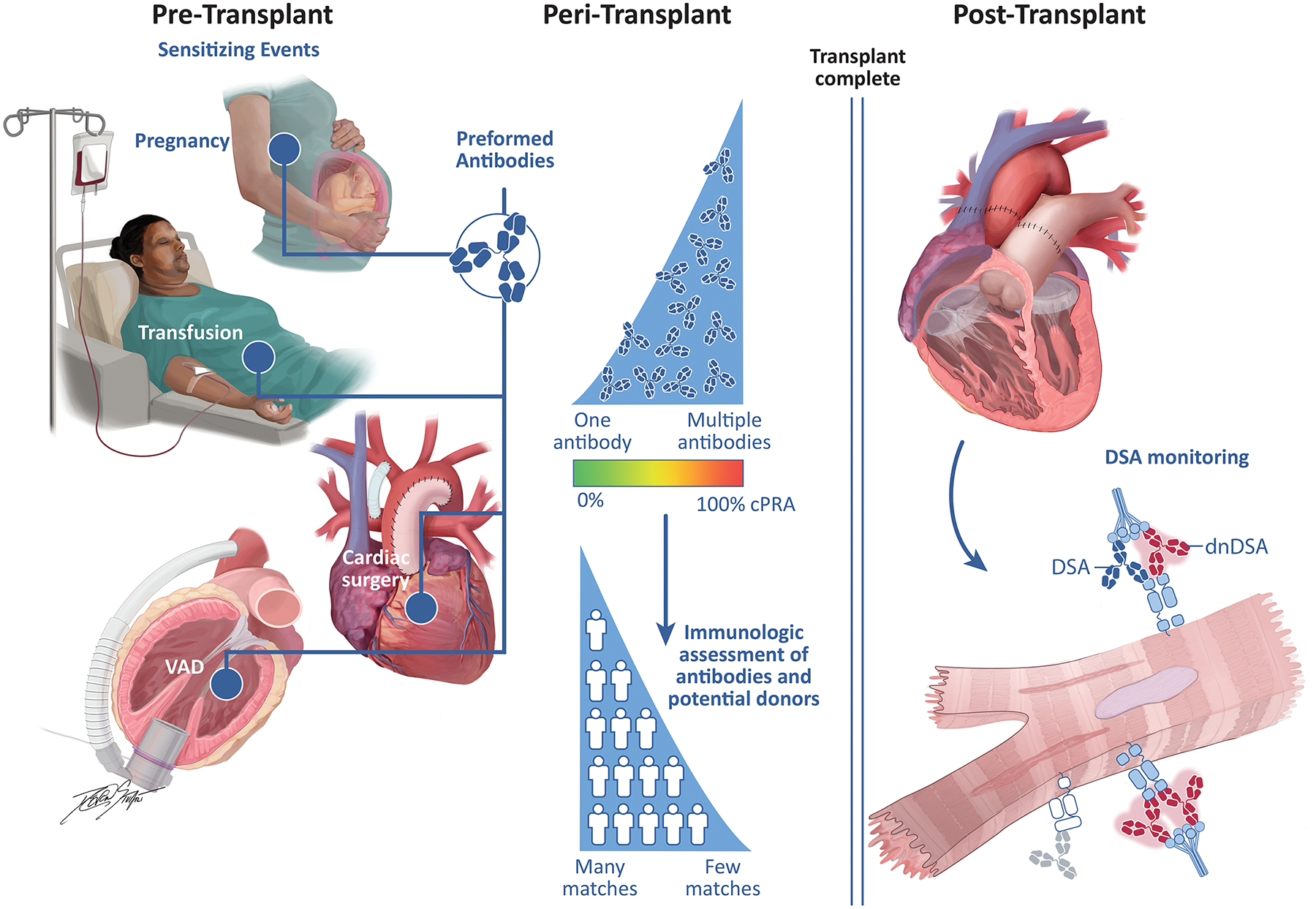
The number of heart transplants performed annually in the United States and worldwide continues to increase, but there has been little change in graft longevity and patient survival over the past 2 decades. The reference standard for diagnosis of acute cellular and antibody-mediated rejection includes histologic and immunofluorescence evaluation of endomyocardial biopsy samples, despite invasiveness and high interrater variability for grading histologic rejection. Circulating biomarkers and molecular diagnostics have shown substantial predictive value in rejection monitoring, and emerging data support their use in diagnosing other posttransplant complications. The use of genomic (cell-free DNA), transcriptomic (mRNA and microRNA profiling), and proteomic (protein expression quantitation) methodologies in diagnosis of these posttransplant outcomes has been evaluated with varying levels of evidence. In parallel, growing knowledge about the genetically mediated immune response leading to rejection (immunogenetics) has enhanced understanding of antibody-mediated rejection, associated graft dysfunction, and death. Antibodies to donor human leukocyte antigens and the technology available to evaluate these antibodies continues to evolve. This review aims to provide an overview of biomarker and immunologic tests used to diagnose posttransplant complications. This includes a discussion of pediatric heart transplantation and the disparate rates of rejection and death experienced by Black patients receiving a heart transplant. This review describes diagnostic modalities that are available and used after transplant and the landscape of future investigations needed to enhance patient outcomes after heart transplantation.
美国和全球每年进行的心脏移植数量持续增加,但在过去的 20 年中,移植物的寿命和患者的生存率几乎没有变化。急性细胞和抗体介导排斥反应的诊断参考标准包括心内膜心肌活检样本的组织学和免疫荧光评估,尽管组织学排斥反应的分级具有侵袭性和高观察者间变异性。循环生物标志物和分子诊断在排斥监测中显示出很大的预测价值,新出现的数据支持它们在诊断其他移植后并发症中的应用。基因组(游离 DNA)、转录组(mRNA 和 microRNA 分析)和蛋白质组(蛋白质表达定量)方法在这些移植后结果的诊断中的应用已经在不同的证据水平上进行了评估。与此同时,对导致排斥的遗传介导免疫反应(免疫遗传学)的认识不断提高,增强了对抗体介导排斥、相关移植物功能障碍和死亡的理解。针对供体人类白细胞抗原的抗体和评估这些抗体的技术不断发展。这篇综述旨在概述用于诊断移植后并发症的生物标志物和免疫测试。这包括讨论儿科心脏移植以及接受心脏移植的黑人患者经历的排斥反应和死亡的差异率。该综述描述了移植后可用和使用的诊断方式,以及未来需要进行哪些研究来改善心脏移植后的患者预后。