Department of Neurology, Albert Einstein College of Medicine, Bronx, NY, USA.
Vector Psychometric Group, LLC, Chapel Hill, NC, USA.
J Neurol. 2023 Dec;270(12):5692-5710. doi: 10.1007/s00415-023-11880-2. Epub 2023 Aug 24.
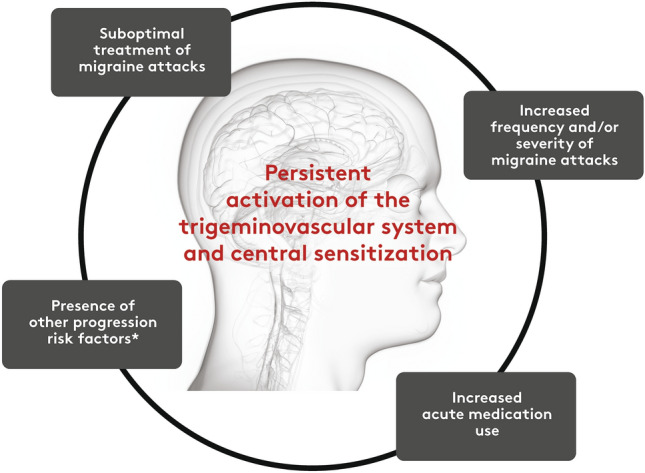
In individuals with migraine, attacks may increase in frequency, severity, or both. Preventing migraine progression has emerged as a treatment goal in headache subspecialty practice, but there may be less awareness in general neurology or primary care settings where most people with migraine who seek treatment consult. Herein, we review the definition of and risk factors for migraine progression and consider strategies that could reduce its risk.
A group of headache expert healthcare professionals, clinicians, and researchers reviewed published evidence documenting factors associated with increased or decreased rates of migraine progression and established expert opinions for disease management recommendations. Strength of evidence was rated as good, moderate, or based solely on expert opinion, using modified criteria for causation developed by AB Hill.
Migraine progression is commonly operationally defined as the transition from ≤ 15 to ≥ 15 monthly headache days among people with migraine; however, this does not necessarily constitute a fundamental change in migraine biology and other definitions should be considered. Established and theoretical key risk factors for migraine progression were categorized into five domains: migraine disease characteristics, treatment-related factors, comorbidities, lifestyle/exogenous factors, and demographic factors. Within these domains, good evidence supports the following risk factors: poorly optimized acute headache treatment, cutaneous allodynia, acute medication overuse, selected psychiatric symptoms, extra-cephalic chronic pain conditions, metabolism-related comorbidities, sleep disturbances, respiratory conditions, former/current high caffeine intake, physical inactivity, financial constraints, tobacco use, and personal triggers as risk factors. Protective actions that may mitigate migraine progression are sparsely investigated in published literature; our discussion of these factors is primarily based on expert opinion.
Recognizing risk factors for migraine progression will allow healthcare providers to suggest protective actions against migraine progression (Supplementary Fig. 1). Intervention studies are needed to weight the risk factors and test the clinical benefit of hypothesized mitigation strategies that emerge from epidemiological evidence.
在偏头痛患者中,发作的频率、严重程度或两者都可能增加。预防偏头痛进展已成为头痛亚专科实践中的治疗目标,但在大多数寻求治疗的偏头痛患者就诊的普通神经科或初级保健环境中,可能意识较低。在此,我们回顾了偏头痛进展的定义和危险因素,并考虑了降低其风险的策略。
一组头痛专家医疗保健专业人员、临床医生和研究人员审查了已发表的证据,这些证据记录了与偏头痛进展率增加或降低相关的因素,并为疾病管理建议建立了专家意见。使用 AB Hill 制定的因果关系修正标准,将证据强度评为良好、中等或仅基于专家意见。
偏头痛进展通常在操作上定义为偏头痛患者从每月 ≤ 15 次头痛日过渡到每月 ≥ 15 次头痛日;然而,这并不一定构成偏头痛生物学的根本变化,应考虑其他定义。偏头痛进展的既定和理论关键风险因素分为五个领域:偏头痛疾病特征、治疗相关因素、合并症、生活方式/外源性因素和人口统计学因素。在这些领域中,有良好证据支持以下风险因素:急性头痛治疗优化不佳、皮肤痛觉过敏、急性药物过度使用、选定的精神症状、颅外慢性疼痛状况、与代谢相关的合并症、睡眠障碍、呼吸状况、既往/当前高咖啡因摄入、身体活动不足、经济限制、吸烟和个人触发因素作为风险因素。预防偏头痛进展的保护措施在已发表的文献中研究甚少;我们对这些因素的讨论主要基于专家意见。
认识到偏头痛进展的危险因素将使医疗保健提供者能够提出预防偏头痛进展的保护措施(补充图 1)。需要进行干预研究,权衡危险因素,并测试从流行病学证据中出现的假设缓解策略的临床获益。