Department of Intensive Care Medicine, Fiona Stanley Hospital, Perth, WA, Robin Warren Drive, 6150, Australia.
University of Western Australia, Perth, WA, 6009, Australia.
Intern Emerg Med. 2023 Oct;18(7):2019-2028. doi: 10.1007/s11739-023-03397-3. Epub 2023 Aug 28.
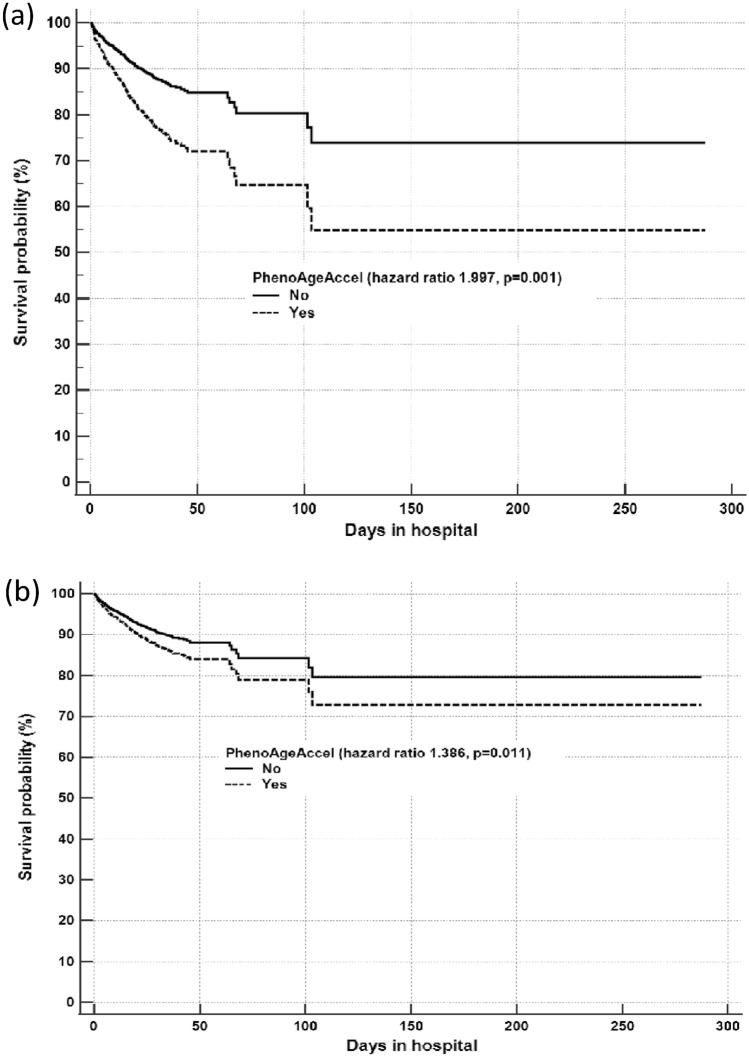
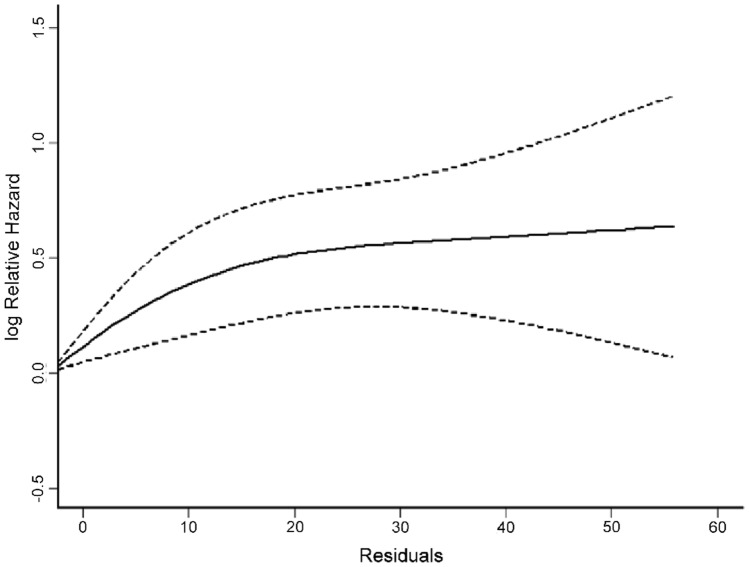
Biological age is increasingly recognized as being more accurate than chronological age in determining chronic health outcomes. This study assessed whether biological age, assessed on intensive care unit (ICU) admission, can predict hospital mortality. This retrospective cohort study, conducted in a tertiary multidisciplinary ICU in Western Australia, used the Levine PhenoAge model to estimate each patient's biological age (also called PhenoAge). Each patient's PhenoAge was calibrated to generate a regression residual which was equivalent to biological age unexplained by chronological age in the local context. PhenoAgeAccel was a dichotomized measure of the residuals, and its presence suggested that one was biologically older than the corresponding chronological age. Of the 2950 critically ill adult patients analyzed, 291 died (9.9%) before hospital discharge. Both PhenoAge and its residuals (after regressing on chronological age) had a significantly better ability to differentiate between hospital survivors and non-survivors than chronological age (area under the receiver-operating-characteristic curve 0.648 and 0.654 vs. 0.547 respectively). Being phenotypically older than one's chronological age was associated with an increased risk of mortality (PhenoAgeAccel hazard ratio [HR] 1.997, 95% confidence interval [CI] 1.568-2.542; p = 0.001) in a dose-related fashion and did not reach a plateau until at least a 20-year gap. This adverse association remained significant (adjusted HR 1.386, 95% CI 1.077-1.784; p = 0.011) after adjusted for severity of acute illness and comorbidities. PhenoAgeAccel was more prevalent among those with pre-existing chronic cardiovascular disease, end-stage renal failure, cirrhosis, immune disease, diabetes mellitus, or those treated with immunosuppressive therapy. Being phenotypically older than one's chronological age was more common among those with comorbidities, and this was associated with an increased risk of mortality in a dose-related fashion in the critically ill that was not fully explained by comorbidities and severity of acute illness.
生物年龄在预测慢性健康结果方面比实际年龄更准确,这一观点已逐渐被人们所认可。本研究旨在评估在重症监护病房(ICU)入院时评估的生物年龄是否可以预测医院死亡率。这是一项在澳大利亚西部一家三级多学科 ICU 进行的回顾性队列研究,研究使用 Levine PhenoAge 模型来评估每位患者的生物年龄(也称为 PhenoAge)。每位患者的 PhenoAge 经过校准以生成回归残差,该残差等效于当地背景下由实际年龄无法解释的生物年龄。PhenoAgeAccel 是残差的二分度量指标,其存在表明患者的生物年龄比实际年龄大。在分析的 2950 名危重症成年患者中,有 291 名患者在出院前死亡(9.9%)。与实际年龄相比,PhenoAge 及其残差(在回归实际年龄后)在区分医院幸存者和非幸存者方面具有更好的区分能力(受试者工作特征曲线下面积分别为 0.648 和 0.654 与 0.547)。表型上比实际年龄大与死亡率增加相关(PhenoAgeAccel 风险比 [HR] 1.997,95%置信区间 [CI] 1.568-2.542;p=0.001),且呈剂量依赖性,至少在相差 20 岁之前仍未达到平台期。在调整急性疾病严重程度和合并症后,这种不良关联仍然显著(调整后的 HR 1.386,95%CI 1.077-1.784;p=0.011)。PhenoAgeAccel 在患有预先存在的慢性心血管疾病、终末期肾衰竭、肝硬化、自身免疫性疾病、糖尿病或接受免疫抑制治疗的患者中更为常见。与实际年龄相比,表型上更老的患者更常见于合并症患者,且这种情况与危重症患者死亡率呈剂量依赖性增加相关,这种增加不能完全由合并症和急性疾病严重程度来解释。