The Spine and Nerve Center of the Virginias, Charleston, WV, USA.
Brigham & Women's Hospital, Boston, MA, USA.
Neuromodulation. 2023 Oct;26(7):1387-1399. doi: 10.1016/j.neurom.2023.07.009. Epub 2023 Aug 28.
Spinal cord stimulation (SCS) is effective for relieving chronic intractable pain conditions. The Dorsal spInal cord STImulatioN vs mediCal management for the Treatment of low back pain study evaluates the effectiveness of SCS compared with conventional medical management (CMM) in the treatment of chronic low back pain in patients who had not undergone and were not candidates for lumbar spine surgery.
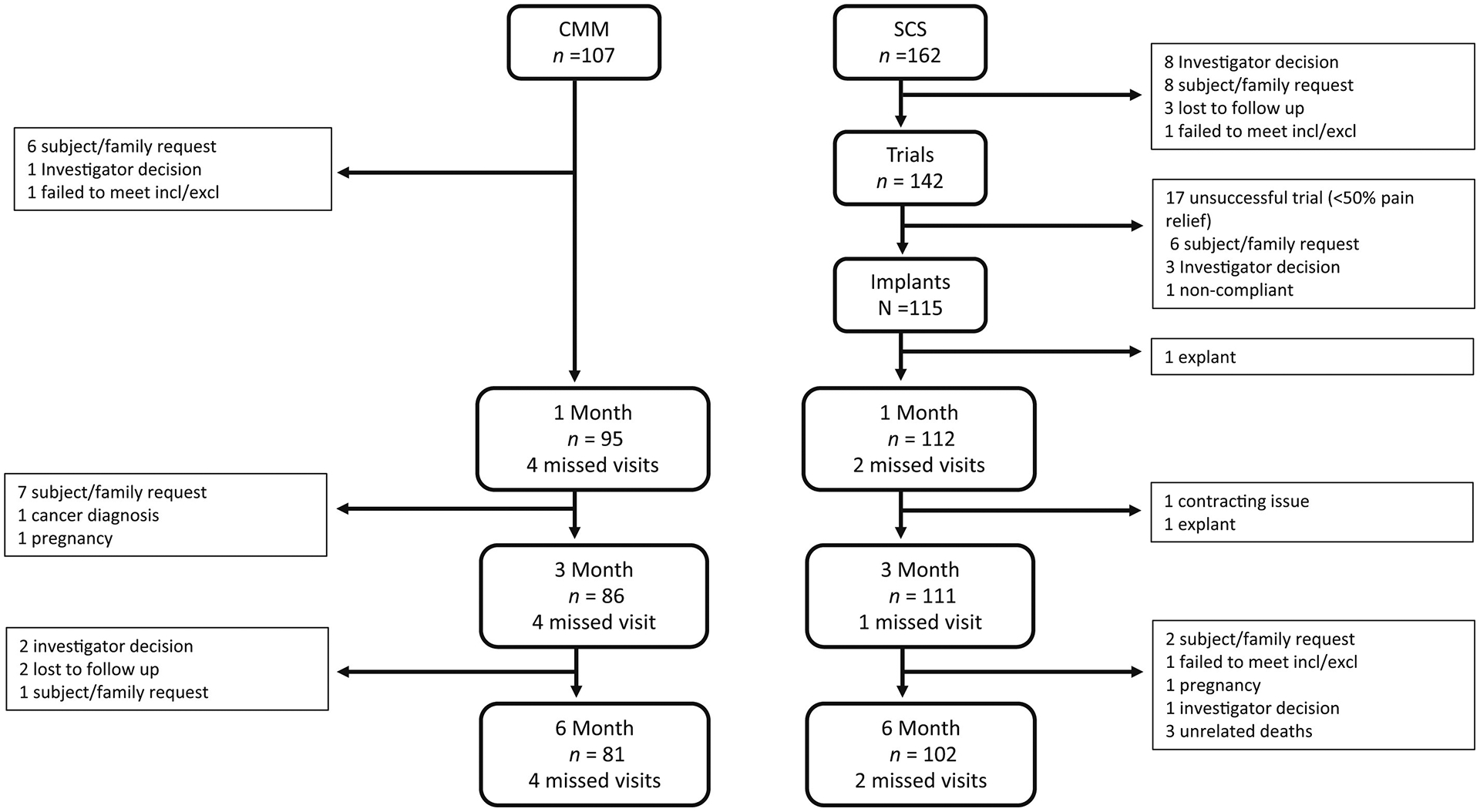
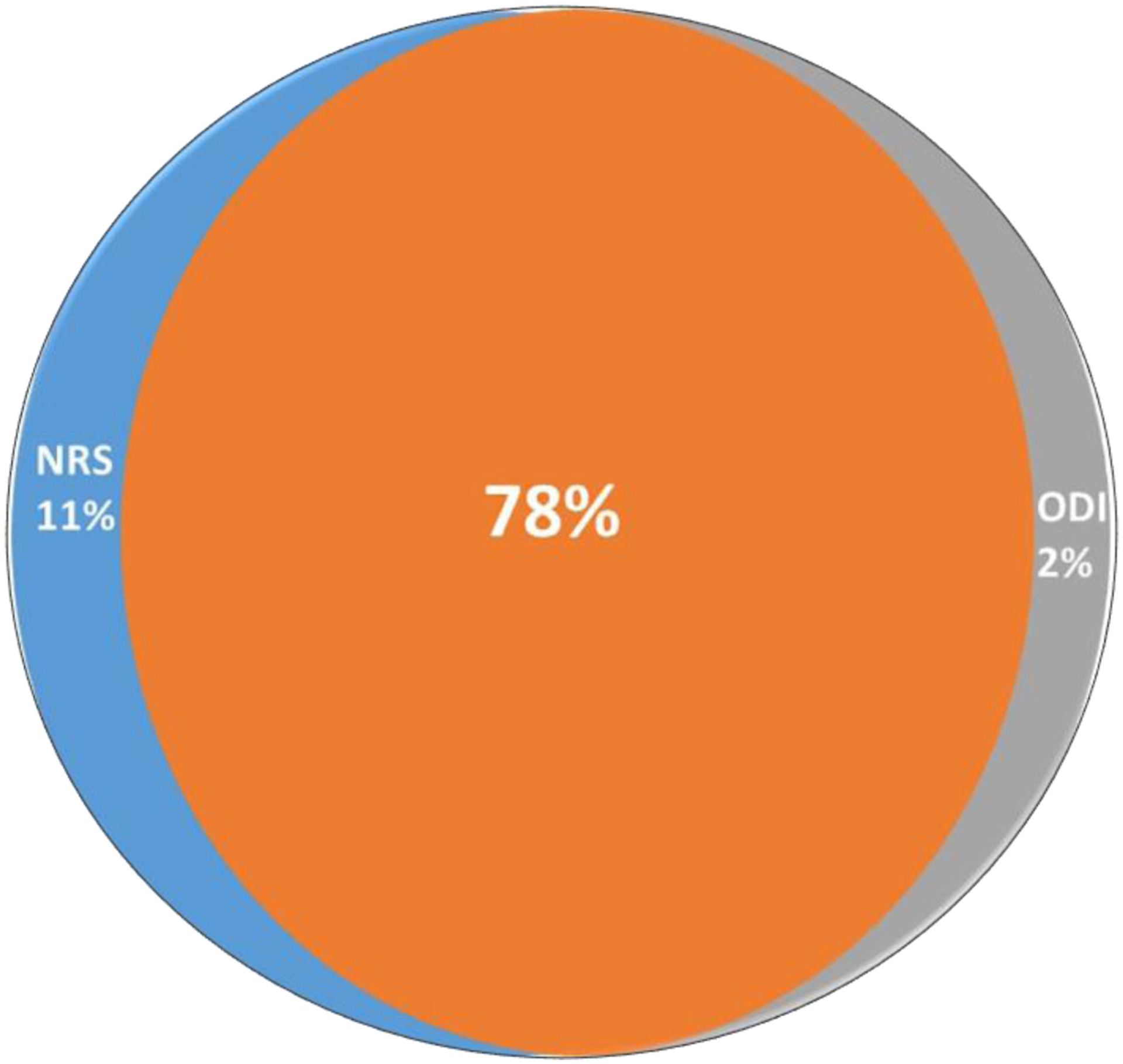
Patients were randomized to passive recharge burst therapy (n = 162) or CMM (n = 107). They reported severe pain and disability for more than a decade and had failed a multitude of therapies. Common diagnoses included degenerative disc disease, spondylosis, stenosis, and scoliosis-yet not to a degree amenable to surgery. The six-month primary end point compared responder rates, defined by a 50% reduction in pain. Hierarchical analyses of seven secondary end points were performed in the following order: composite responder rate (numerical rating scale [NRS] or Oswestry Disability Index [ODI]), NRS, ODI, Pain Catastrophizing Scale responder rate, Patient Global Impression of Change (PGIC) responder rate, and Patient-Reported Outcome Measure Information System-29 in pain interference and physical function.
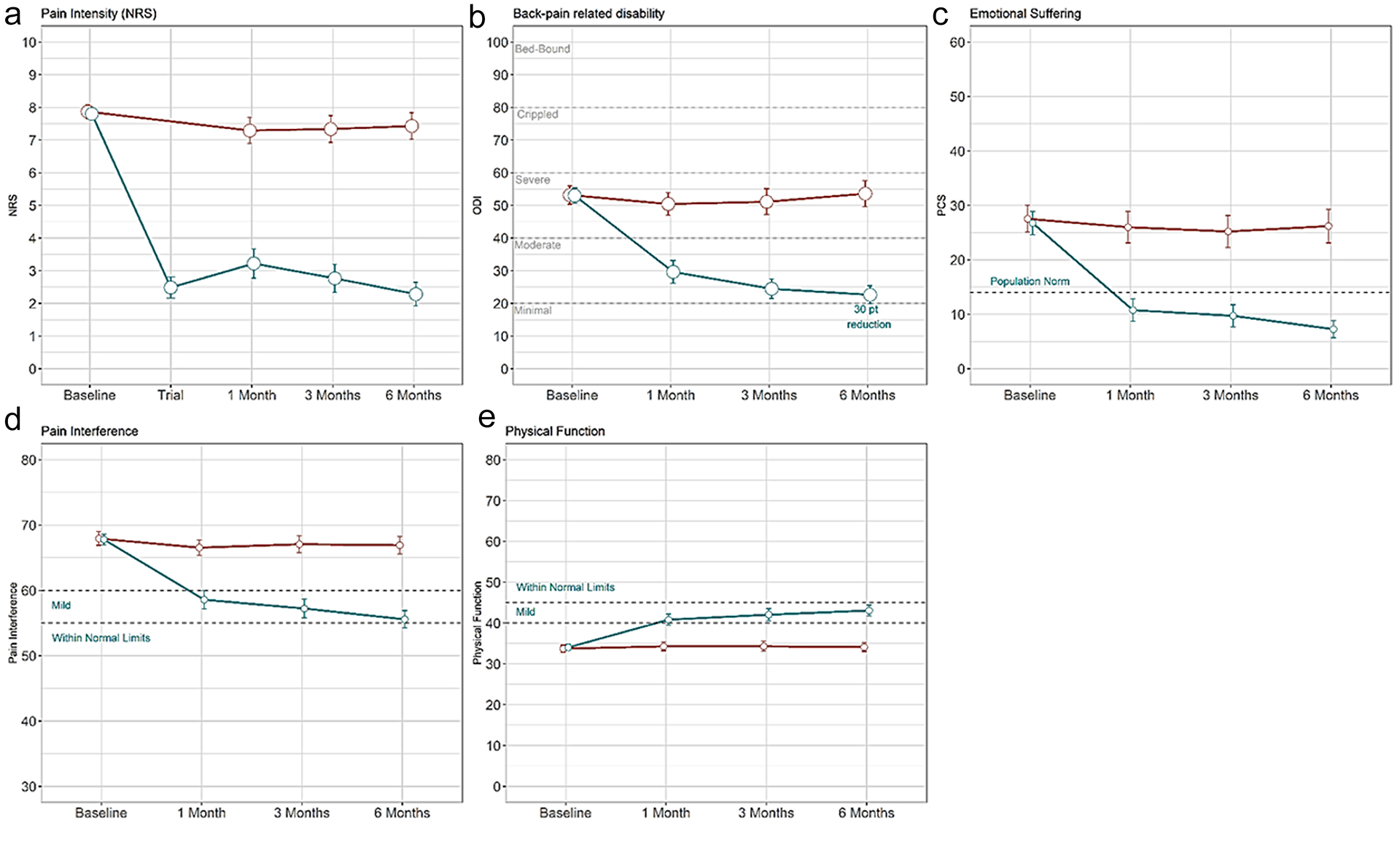
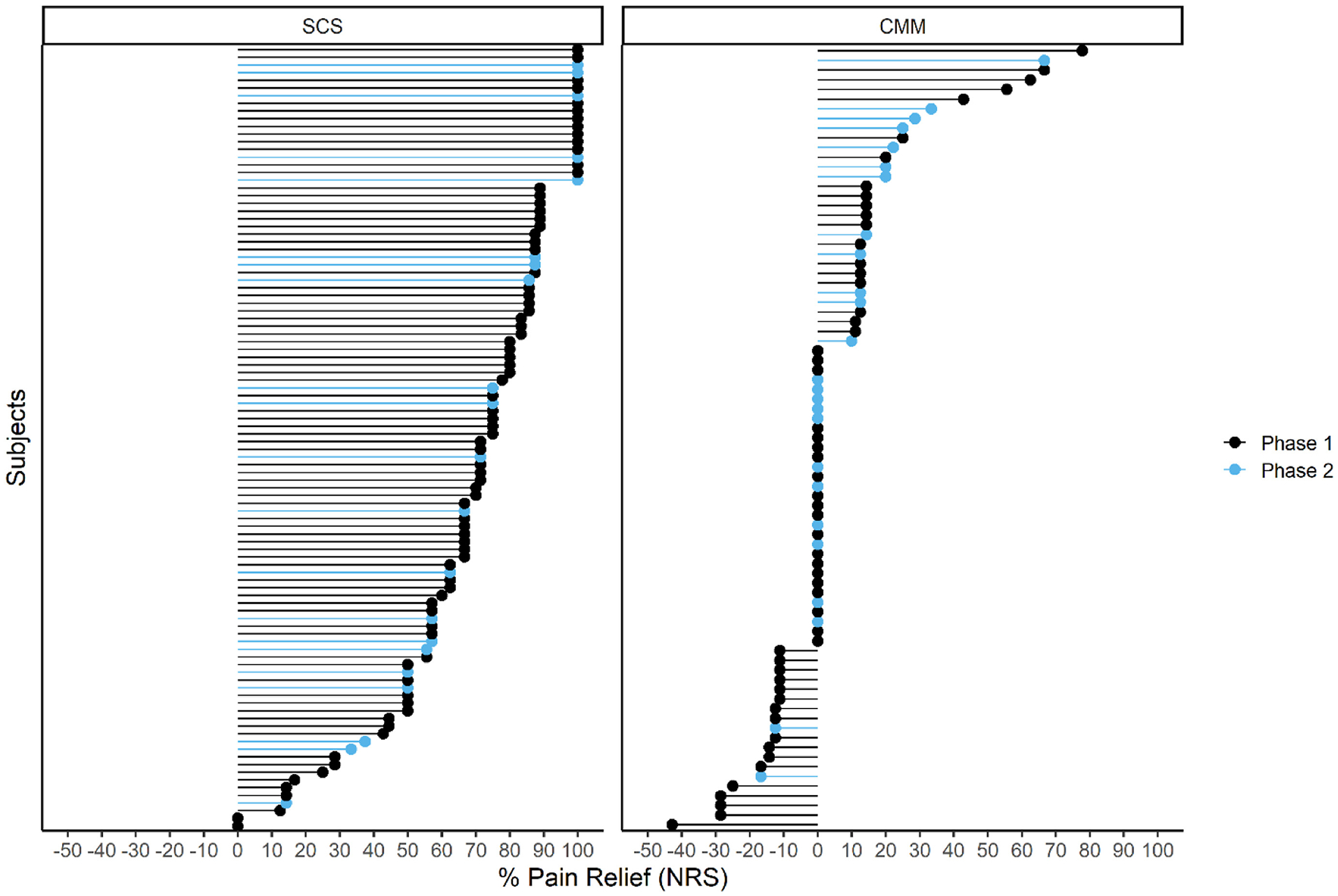
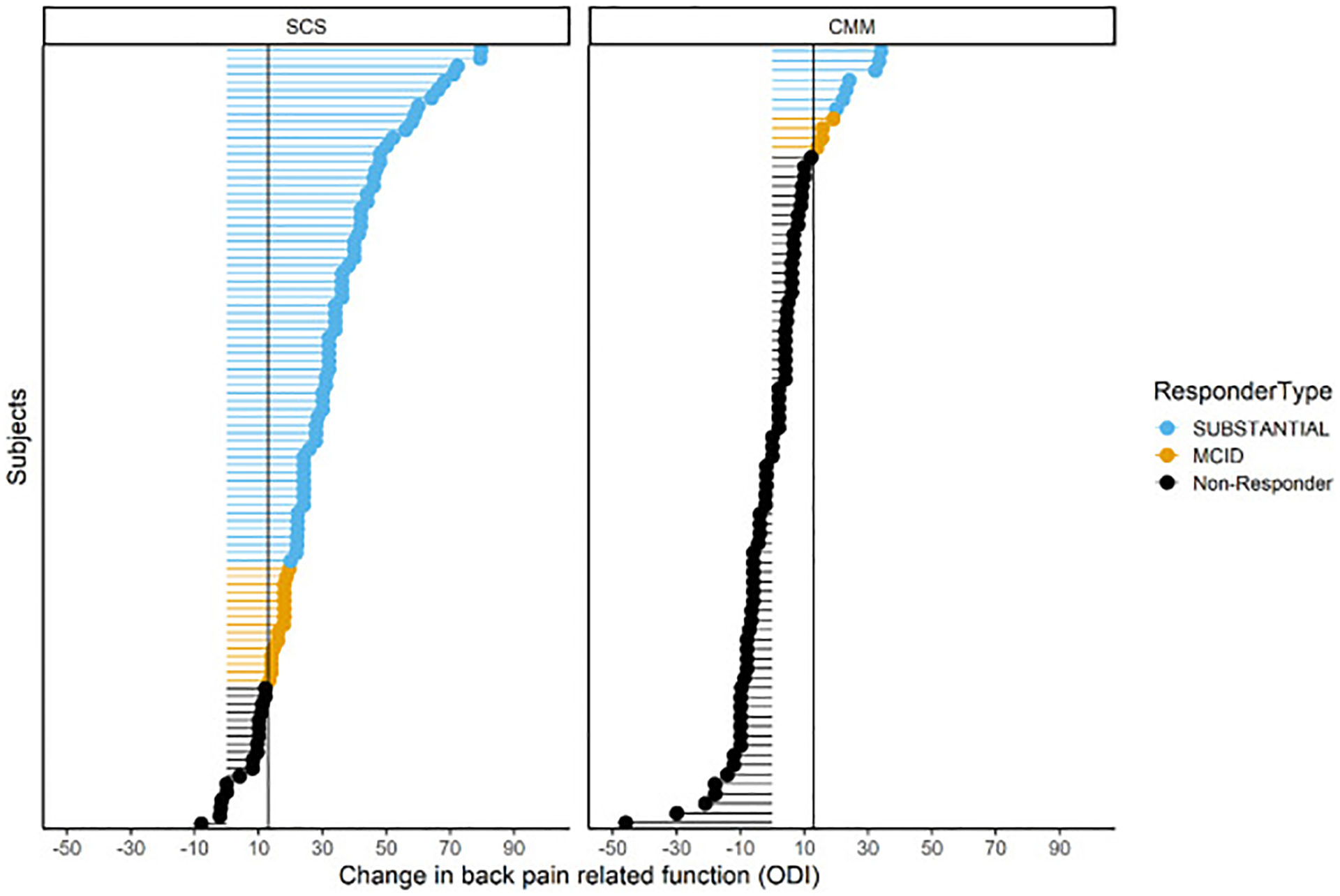
Intention-to-treat analysis showed a significant difference in pain responders on NRS between SCS (72.6%) and CMM (7.1%) arms (p < 0.0001). Of note, 85.2% of those who received six months of therapy responded on NRS compared with 6.2% of those with CMM (p < 0.0001). All secondary end points indicated the superiority of burst therapy over CMM. A composite measure on function or pain relief showed 91% of subjects with SCS improved, compared with 16% of subjects with CMM. A substantial improvement of 30 points was observed on ODI compared with a <one-point change in the CMM arm. Three serious and 14 non-serious device- or procedure-related events were reported.
This study found substantial improvement at six months in back pain, back pain-related disability, pain-related emotional suffering, PGIC, pain interference, and physical function in a population with severe, debilitating back pain for more than a decade. These improvements were reported in conjunction with reduced opioid use, injection, and ablation therapy.
The Clinicaltrials.gov registration number for the study is NCT04479787.
脊髓刺激(SCS)对缓解慢性难治性疼痛疾病有效。Dorsal spInal cord STImulatioN vs mediCal management for the Treatment of low back pain 研究评估了 SCS 与常规医疗管理(CMM)治疗慢性腰痛的疗效,该研究纳入了未经腰椎手术且不符合手术条件的慢性腰痛患者。
患者被随机分为被动充电爆发治疗组(n=162)或 CMM 组(n=107)。他们报告说,疼痛和残疾已经持续了十多年,并且已经尝试了多种治疗方法但都失败了。常见的诊断包括退行性椎间盘疾病、颈椎病、狭窄症和脊柱侧凸,但还没有到可以手术的程度。六个月的主要终点比较了应答率,应答定义为疼痛减轻 50%。对七个次要终点进行了分层分析,顺序如下:综合应答率(数字评分量表[NRS]或 Oswestry 残疾指数[ODI])、NRS、ODI、疼痛灾难化量表应答率、患者总体印象变化(PGIC)应答率以及患者报告结局测量信息系统-29 疼痛干扰和身体功能。
意向治疗分析显示,SCS(72.6%)和 CMM(7.1%)组在 NRS 上的疼痛应答者之间存在显著差异(p<0.0001)。值得注意的是,与 CMM 组的 6.2%相比,接受 6 个月治疗的患者中,有 85.2%的患者在 NRS 上有应答(p<0.0001)。所有次要终点均表明爆发治疗优于 CMM。功能或疼痛缓解的综合测量显示,91%的 SCS 组患者得到改善,而 CMM 组只有 16%的患者得到改善。ODI 观察到 30 分的显著改善,而 CMM 组的变化小于 1 分。报告了 3 例严重和 14 例非严重的设备或程序相关事件。
本研究发现,在患有严重、致残性腰痛超过十年的人群中,在背痛、与背痛相关的残疾、与疼痛相关的情绪困扰、PGIC、疼痛干扰和身体功能方面,在六个月时均有明显改善。这些改善伴随着阿片类药物使用、注射和消融治疗的减少。
该研究的 Clinicaltrials.gov 注册号为 NCT04479787。