White Thomas, Justiz Rafael, Almonte Wilson, Micovic Velimir, Shah Binit, Anderson Eric, Kapural Leonardo, Cordner Harold, El-Naggar Amr, Fishman Michael, Eshraghi Yashar, Kim Philip, Abd-Elsayed Al, Chakravarthy Krishnan, Millet Yoann, Sanapati Mahendra, Harrison Nathan, Goff Brandon, Gupta Mayank, Grewal Prabhdeep, Wilkinson Michael, Bundschu Richard, Will Andrew, Satija Pankaj, Li Sean, Dulebohn Scott, Broadnax John, Gekht Gennady, Wu Ken, Falowski Steven, Park Wesley, Cedeno David L, Vallejo Ricardo
Procura Pain and Spine, Pain Management. 111 Vision Park Blvd #100, Shenandoah, TX 77384.
Oklahoma Pain Physicians, Pain Management, 4117 NW 122nd St #C, Oklahoma City, OK 73120.
N Am Spine Soc J. 2024 Jul 17;19:100528. doi: 10.1016/j.xnsj.2024.100528. eCollection 2024 Sep.
Successful treatments for intractable chronic low back pain (CLBP) in patients who are not eligible for surgical interventions are scarce. The superior efficacy of differential target multiplexed spinal cord stimulation (DTM SCS) to conventional SCS (Conv-SCS) on the treatment of CLBP in patients with persistent spinal pain syndrome (PSPS) who have failed surgical interventions (PSPS-T2) motivated the evaluation of DTM SCS versus Conv-SCS on PSPS patients who are non-surgical candidates (PSPS-T1).
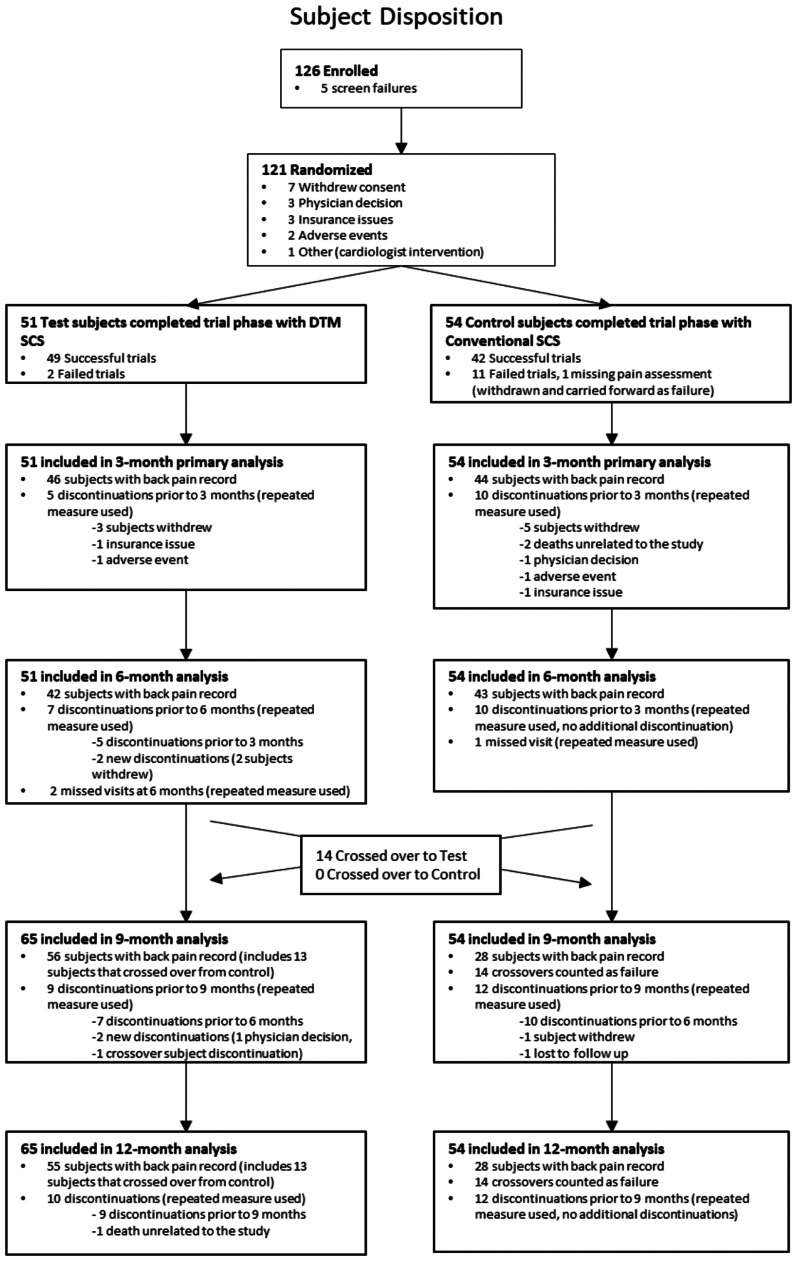
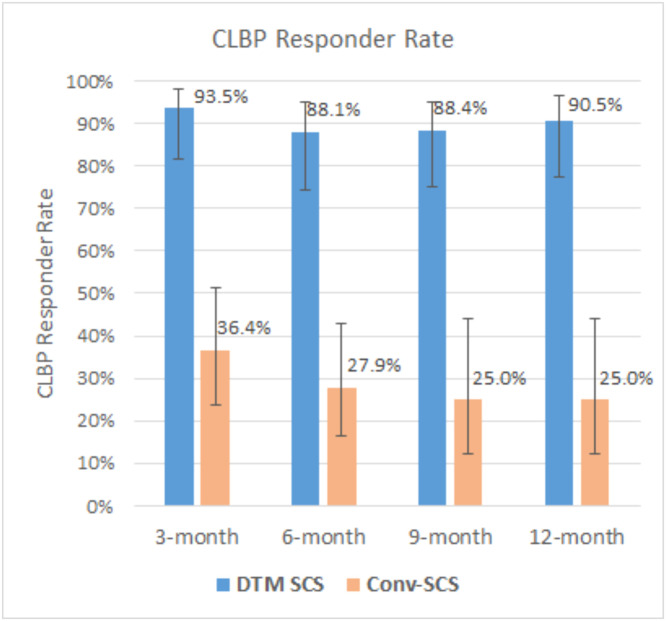
This is a prospective, open label, crossover, post-market randomized controlled trial in 20 centers across the United States. Eligible patients were randomized to either DTM SCS or Conv-SCS in a 1:1 ratio. Primary endpoint was CLBP responder rate (percentage of subjects with ≥50% CLBP relief) at 3-month in randomized subjects who completed trialing (modified intention-to-treat population). Patients were followed up to 12 months. Secondary endpoints included change of CLBP and leg pain, responder rates, changes in disability, quality of life, patient satisfaction and global impression of change, and safety profile. An optional crossover was available at 6-month to all patients.
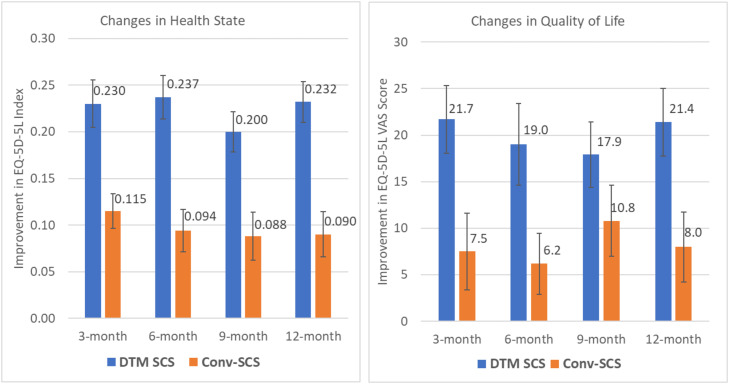
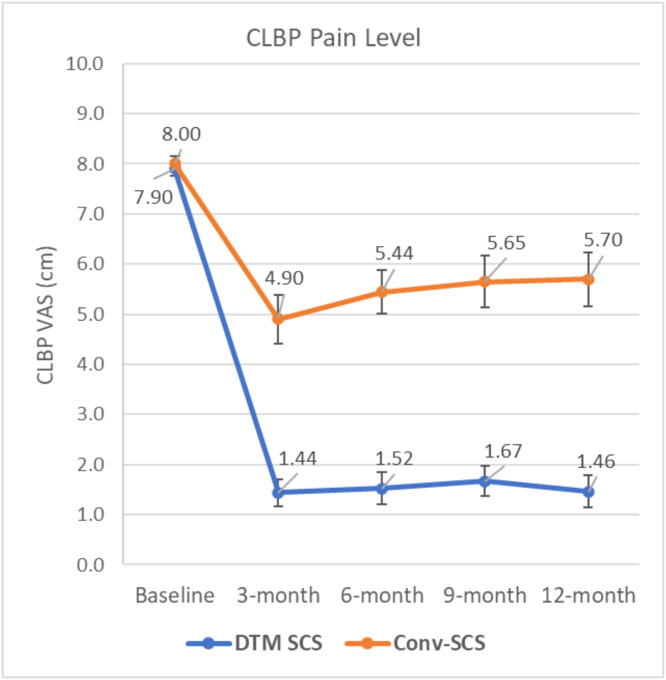
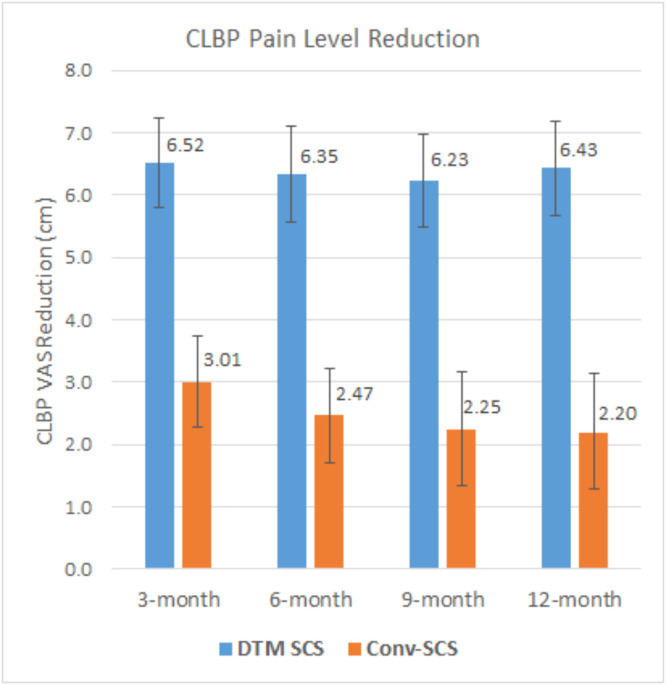
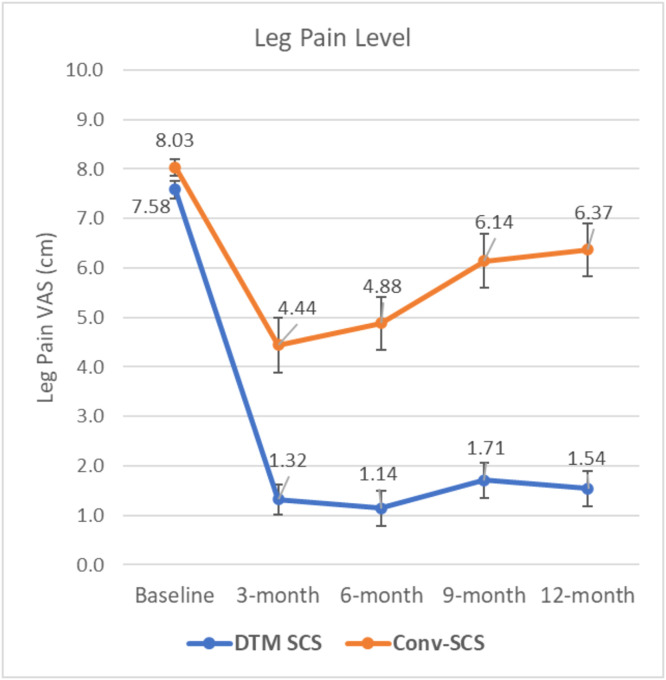
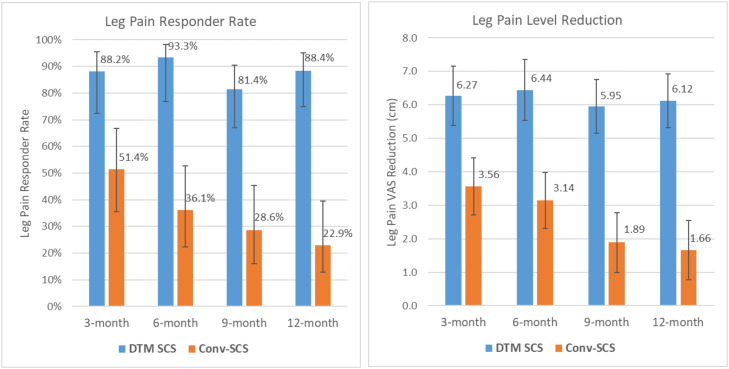
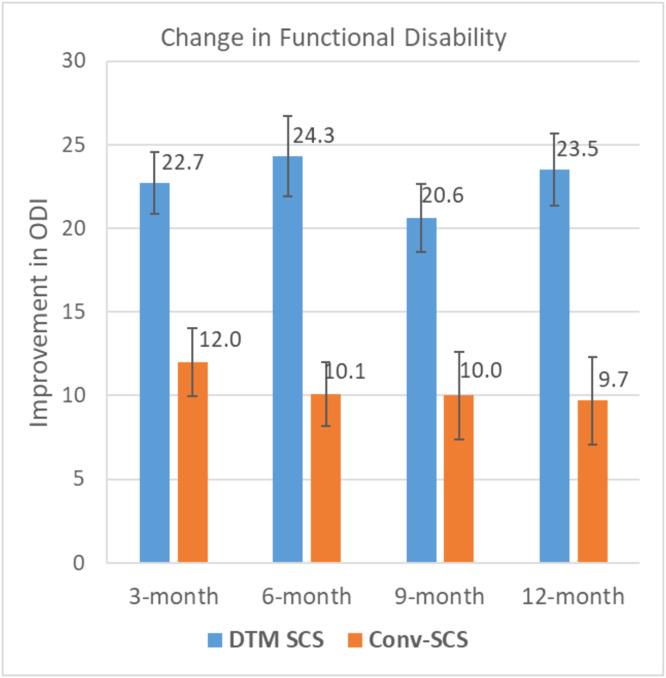
About 121 PSPS-T1 subjects with CLBP and leg pain mostly associated with degenerative disc disease and radiculopathy and who were not eligible for spine surgery were randomized. CLBP responder rate with DTM SCS (93.5%) was superior to Conv-SCS (36.4%) at the primary endpoint. Superior CLBP responder rates (88.1%-90.5%) were obtained with DTM SCS at all other timepoints. Mean CLBP reduction with DTM SCS (6.52 cm) was superior to that with Conv-SCS (3.01 cm) at the primary endpoint. Similar CLBP reductions (6.23-6.43 cm) were obtained with DTM SCS at other timepoints. DTM SCS provided significantly better leg pain reduction and responder rate, improvement of disability and quality of life, and better patient satisfaction and global impression of change. 90.9% of Conv-SCS subjects who crossed over were CLBP responders at completion of the study. Similar safety profiles were observed between the two groups.
DTM SCS for chronic CLBP in nonsurgical candidates is superior to Conv-SCS. Improvements were sustained and provided significant benefits on the management of these patients.
对于不适合手术干预的顽固性慢性腰痛(CLBP)患者,成功的治疗方法很少。在手术干预失败的持续性脊柱疼痛综合征(PSPS)患者(PSPS-T2)中,差异靶点多重脊髓刺激(DTM SCS)治疗CLBP的疗效优于传统脊髓刺激(Conv-SCS),这促使我们对DTM SCS与Conv-SCS在非手术候选的PSPS患者(PSPS-T1)中的疗效进行评估。
这是一项在美国20个中心进行的前瞻性、开放标签、交叉、上市后随机对照试验。符合条件的患者按1:1的比例随机分为DTM SCS组或Conv-SCS组。主要终点是在完成试验的随机受试者中(改良意向性治疗人群),3个月时CLBP缓解率(CLBP缓解≥50%的受试者百分比)。对患者进行长达12个月的随访。次要终点包括CLBP和腿痛的变化、缓解率、残疾程度、生活质量、患者满意度和总体变化印象以及安全性。所有患者在6个月时可选择交叉治疗。
约121例患有CLBP和腿痛的PSPS-T1受试者被随机分组,这些疼痛大多与椎间盘退变疾病和神经根病相关,且不符合脊柱手术条件。在主要终点,DTM SCS组的CLBP缓解率(93.5%)高于Conv-SCS组(36.4%)。在所有其他时间点,DTM SCS组的CLBP缓解率均较高(88.1%-90.5%)。在主要终点,DTM SCS组的平均CLBP降低幅度(6.52 cm)优于Conv-SCS组(3.01 cm)。在其他时间点,DTM SCS组的CLBP降低幅度相似(6.23-6.43 cm)。DTM SCS在减轻腿痛和缓解率、改善残疾程度和生活质量、提高患者满意度和总体变化印象方面明显更优。90.9%交叉至DTM SCS组的Conv-SCS组受试者在研究结束时成为CLBP缓解者。两组观察到相似的安全性。
对于非手术候选的慢性CLBP患者,DTM SCS优于Conv-SCS。改善效果持续存在,为这些患者的治疗带来显著益处。