Yue James J, Gilligan Christopher J, Falowski Steven, Jameson Jessica, Desai Mehul J, Moeschler Susan, Pilitsis Julie, Heros Robert, Tavel Edward, Wahezi Sayed, Funk Robert, Buchanan Patrick, Christopher Anne, Weisbein Jacqueline, Patterson Denis, Levy Robert, Antony Ajay, Miller Nathan, Scarfo Keith, Kreiner Scott, Wilson Derron, Lim Chi, Braun Edward, Dickerson David, Duncan Jonathan, Xu Jijun, Candido Kenneth, Mohab Ibrahim, Michael Fishell, Blomme Bram, Okaro Udoka, Deer Timothy
Connecticut Orthopaedics, Hamden, CT, United States.
Brigham and Women's Hospital, Boston, MA, United States.
N Am Spine Soc J. 2024 Jun 21;19:100508. doi: 10.1016/j.xnsj.2024.100508. eCollection 2024 Sep.
Low back pain (LBP) is a highly prevalent, disabling condition affecting millions of people. Patients with an identifiable anatomic pain generator and resulting neuropathic lower extremity symptoms often undergo spine surgery, but many patients lack identifiable and/or surgically corrective pathology. Nonoperative treatment options often fail to provide sustained relief. Spinal cord stimulation (SCS) is sometimes used to treat these patients, but the lack of level 1 evidence limits its widespread use and insurance coverage. The DISTINCT RCT study evaluates the efficacy of passive recharge burst SCS compared to conventional medical treatment (CMM) in alleviating chronic, refractory axial low back pain.
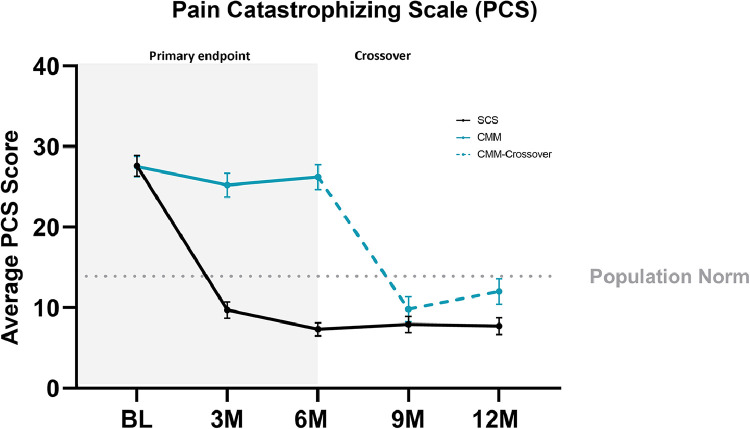
This prospective, multicenter, randomized, study with an optional 6-month crossover involved patients who were not candidates for lumbar spine surgery. The primary and secondary endpoints evaluated improvements in low back pain intensity (NRS), back pain-related disability (ODI), pain catastrophizing (PCS), and healthcare utilization. Patients were randomized to SCS therapy or CMM at 30 US study sites.
The SCS arm reported an 85.3% NRS responder rate (≥ 50% reduction) compared to 6.2% (5/81) in the CMM arm. After the 6M primary endpoint, SCS patients elected to remain on assigned therapy and 66.2% (49/74) of CMM patients chose to trial SCS (crossover). At the 12M follow-up, SCS and crossover patients reported 78.6% and 71.4% NRS responder rates. Secondary outcomes indicated significant improvements in ODI, PCS, and reduced healthcare utilization. Six serious adverse events were reported and resolved without sequelae.
DISTINCT chronic low back pain patients with no indication for corrective surgery experienced a significant and sustained response to burst SCS therapy for up to 12 months. CMM patients who crossed over to the SCS arm reported profound improvements after 6 months. This data advocates for a timely consideration of SCS therapy in patients unresponsive to conservative therapy.
腰痛(LBP)是一种极为常见的致残性疾病,影响着数百万人。患有可识别的解剖性疼痛源并伴有神经性下肢症状的患者通常会接受脊柱手术,但许多患者缺乏可识别的和/或手术可矫正的病理状况。非手术治疗方案往往无法提供持续缓解。脊髓刺激(SCS)有时用于治疗这些患者,但缺乏一级证据限制了其广泛应用和保险覆盖范围。DISTINCT随机对照试验研究评估了被动充电脉冲SCS与传统医学治疗(CMM)相比在缓解慢性难治性轴性腰痛方面的疗效。
这项前瞻性、多中心、随机研究设有一个可选的6个月交叉期,纳入了不适合进行腰椎手术的患者。主要和次要终点评估腰痛强度(数字评分量表,NRS)、背痛相关残疾(Oswestry功能障碍指数,ODI)、疼痛灾难化(疼痛灾难化量表,PCS)以及医疗保健利用情况的改善。患者在美国30个研究地点被随机分配接受SCS治疗或CMM治疗。
SCS组报告的NRS缓解率(降低≥50%)为85.3%,而CMM组为6.2%(5/81)。在6个月的主要终点之后,SCS组患者选择继续接受指定治疗,66.2%(49/74)的CMM组患者选择试用SCS(交叉)。在12个月的随访中,SCS组和交叉组患者报告的NRS缓解率分别为78.6%和71.4%。次要结果表明ODI、PCS有显著改善,医疗保健利用减少。报告了6起严重不良事件且均已解决,无后遗症。
DISTINCT研究中无矫正手术指征的慢性腰痛患者对脉冲SCS治疗有显著且持续的反应,长达12个月。交叉至SCS组的CMM组患者在6个月后报告有显著改善。这些数据支持对保守治疗无反应的患者及时考虑SCS治疗。