Gaieski David F, Tsukuda Jumpei, Maddox Parker, Li Michael
Sidney Kimmel Medical College, Thomas Jefferson University, Philadelphia, PA.
Department of Emergency Medicine, Thomas Jefferson University, Philadelphia, PA.
Crit Care Explor. 2023 Aug 25;5(9):e0964. doi: 10.1097/CCE.0000000000000964. eCollection 2023 Sep.
We analyzed whether patients with the International Classification of Diseases, 10th Edition (ICD-10) discharge diagnosis code for sepsis are different in regard to demographics and outcome variables when comparing those with sepsis only to those also diagnosed with COVID-19 or those with a COVID-19 diagnosis alone.
Retrospective cohort study.
Nine hospitals in an academic health system.
Patients with a final ICD-10 discharge diagnostic code for sepsis only, a diagnosis of COVID-19-only, or a final sepsis ICD-10 discharge code + a diagnosis of COVID-19 admitted to the hospital were analyzed for demographic and outcome differences between the cohorts.
None.
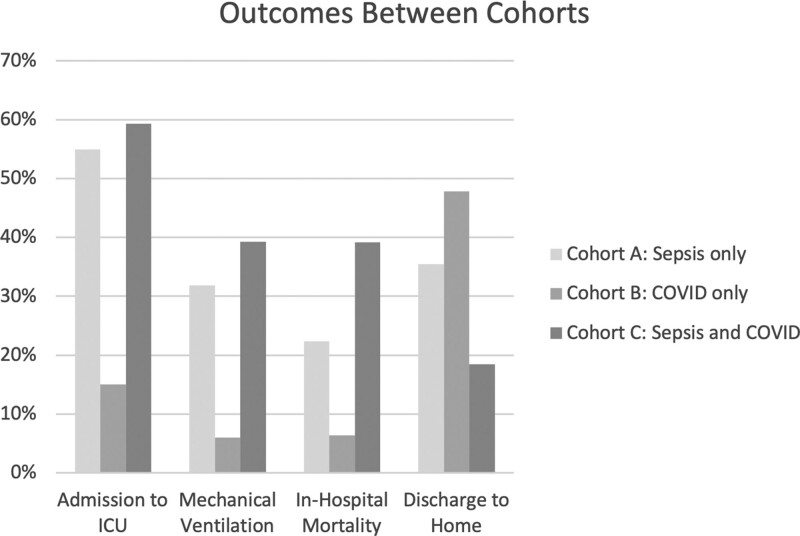
A total of 11,395 patients met inclusion criteria: 6,945 patients (60.9%) were ICD-10 sepsis code only, 3,294 patients (28.9%) were COVID-19 diagnosis-only, and 1,153 patients (10.1%) were sepsis ICD-10 code + COVID-19 diagnosis. Comparing sepsis ICD-10 code + COVID-19 diagnosis patients to sepsis ICD-10 code only and COVID-19 diagnosis-only patients, the sepsis ICD-10 code + COVID-19 diagnosis patients were: older (69 [58-78] vs 67 [56-77] vs 64 [51-76] yr), less likely to be female (40.3% vs 46.7% vs 49.5%), more frequently admitted to the ICU (59.3% [684/1,153] vs 54.9% [1,810/3,297] vs 15% [1,042/6,945]), more frequently required ventilatory support (39.3% [453/1,153] vs 31.8% [1,049/3,297] vs 6.0% [417/6,945]), had longer median hospital length of stay (9 [5,16] vs 5 [3,8] vs 7. [4,13] d), and were more likely to die in the hospital (39.2% [452/1,153] vs 22.3% [735/3,297] vs 6.4% [444/6,945]).
During the COVID-19 pandemic the sickest cohort of patients was those receiving an explicit ICD-10 code of sepsis + a COVID-19 diagnosis. A significant percentage of COVID-19 diagnosis-only patients appear to have been under-coded as they received a level of critical care (ICU admission; intubation) suggestive of the presence of acute organ dysfunction during their admission.
我们分析了国际疾病分类第10版(ICD - 10)中败血症出院诊断代码的患者在人口统计学和结局变量方面是否存在差异,具体比较了仅患有败血症的患者与同时诊断为COVID - 19的患者以及仅患有COVID - 19诊断的患者。
回顾性队列研究。
一个学术医疗系统中的九家医院。
对仅具有最终ICD - 10败血症出院诊断代码、仅诊断为COVID - 19或最终败血症ICD - 10出院代码加COVID - 19诊断并入院的患者进行队列间人口统计学和结局差异分析。
无。
共有11395名患者符合纳入标准:6945名患者(60.9%)仅有ICD - 10败血症代码,3294名患者(28.9%)仅有COVID - 19诊断,1153名患者(10.1%)为败血症ICD - 10代码加COVID - 19诊断。将败血症ICD - 10代码加COVID - 19诊断的患者与仅有败血症ICD - 10代码和仅有COVID - 19诊断的患者进行比较,败血症ICD - 10代码加COVID - 19诊断的患者:年龄更大(69[58 - 78]岁 vs 67[56 - 77]岁 vs 64[51 - 76]岁),女性比例更低(40.3% vs 46.7% vs 49.5%),更频繁入住重症监护病房(59.3%[684/1153] vs 54.9%[1810/3297] vs 15%[1042/6945]),更频繁需要通气支持(39.3%[453/1153] vs 31.8%[1049/3297] vs 6.0%[417/6945]),中位住院时间更长(9[5,16]天 vs 5[3,8]天 vs 7[4,13]天),且更有可能在医院死亡(39.2%[452/1153] vs 22.3%[735/3297] vs 6.4%[444/6945])。
在COVID - 19大流行期间,病情最严重的患者群体是那些明确具有ICD - 10败血症代码加COVID - 19诊断的患者。相当一部分仅诊断为COVID - 19的患者似乎编码不足,因为他们在入院期间接受了提示存在急性器官功能障碍的重症监护水平(入住ICU;插管)。