Cardiovascular Department, Guy's and St Thomas' NHS Foundation Trust, London, UK; Cardiovascular Department, Faculty of Life Sciences and Medicine, King's College London, London, UK.
Clinical Trials Unit, Warwick Medical School, University of Warwick, Coventry, UK.
Lancet. 2023 Oct 14;402(10410):1329-1337. doi: 10.1016/S0140-6736(23)01351-X. Epub 2023 Aug 27.
The International Liaison Committee on Resuscitation has called for a randomised trial of delivery to a cardiac arrest centre. We aimed to assess whether expedited delivery to a cardiac arrest centre compared with current standard of care following resuscitated cardiac arrest reduces deaths.
ARREST is a prospective, parallel, multicentre, open-label, randomised superiority trial. Patients (aged ≥18 years) with return of spontaneous circulation following out-of-hospital cardiac arrest without ST elevation were randomly assigned (1:1) at the scene of their cardiac arrest by London Ambulance Service staff using a secure online randomisation system to expedited delivery to the cardiac catheter laboratory at one of seven cardiac arrest centres or standard of care with delivery to the geographically closest emergency department at one of 32 hospitals in London, UK. Masking of the ambulance staff who delivered the interventions and those reporting treatment outcomes in hospital was not possible. The primary outcome was all-cause mortality at 30 days, analysed in the intention-to-treat (ITT) population excluding those with unknown mortality status. Safety outcomes were analysed in the ITT population. The trial was prospectively registered with the International Standard Randomised Controlled Trials Registry, 96585404.
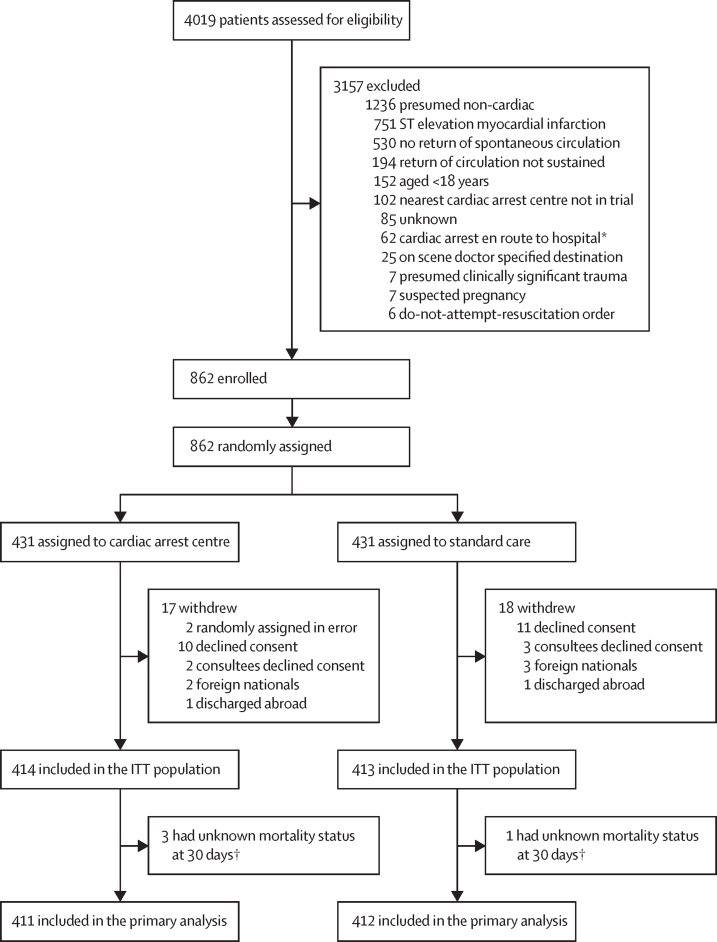
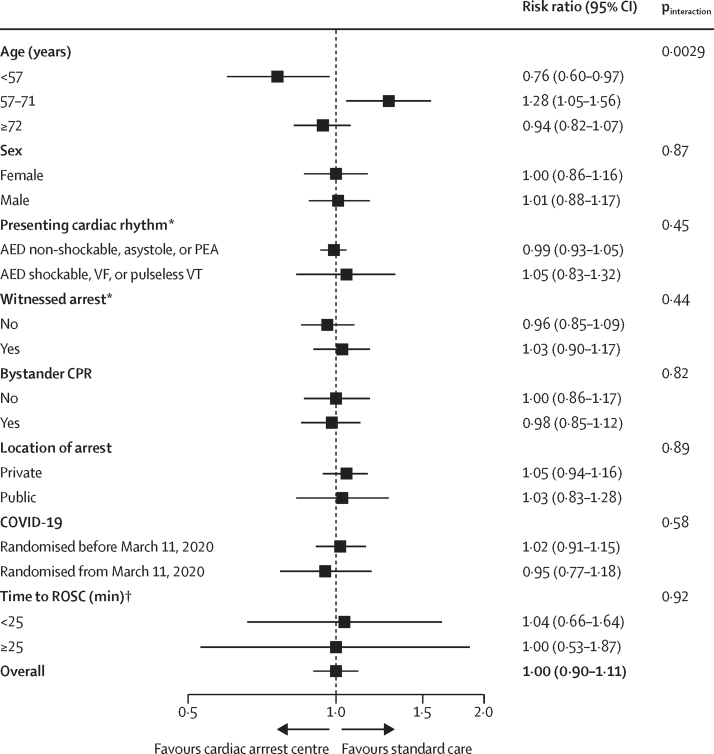
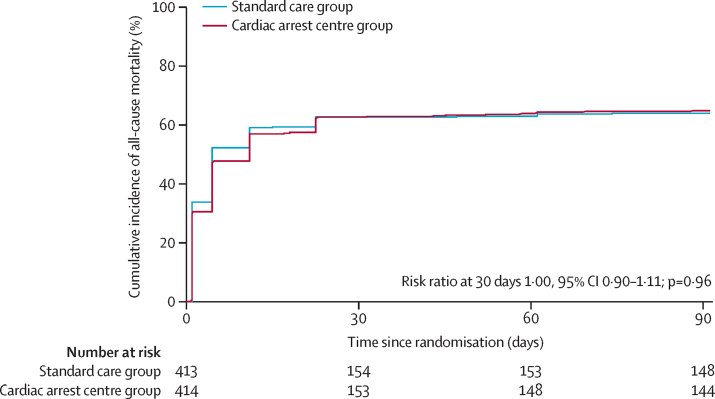
Between Jan 15, 2018, and Dec 1, 2022, 862 patients were enrolled, of whom 431 (50%) were randomly assigned to a cardiac arrest centre and 431 (50%) to standard care. 20 participants withdrew from the cardiac arrest centre group and 19 from the standard care group, due to lack of consent or unknown mortality status, leaving 411 participants in the cardiac arrest centre group and 412 in the standard care group for the primary analysis. Of 822 participants for whom data were available, 560 (68%) were male and 262 (32%) were female. The primary endpoint of 30-day mortality occurred in 258 (63%) of 411 participants in the cardiac arrest centre group and in 258 (63%) of 412 in the standard care group (unadjusted risk ratio for survival 1·00, 95% CI 0·90-1·11; p=0·96). Eight (2%) of 414 patients in the cardiac arrest centre group and three (1%) of 413 in the standard care group had serious adverse events, none of which were deemed related to the trial intervention.
In adult patients without ST elevation, transfer to a cardiac arrest centre following resuscitated cardiac arrest in the community did not reduce deaths.
British Heart Foundation.
国际复苏联络委员会呼吁进行一项将分娩送往心脏骤停中心的随机试验。我们旨在评估与复苏后心脏骤停的当前标准护理相比,将分娩送往心脏骤停中心是否会降低死亡率。
ARREST 是一项前瞻性、平行、多中心、开放标签、随机优势试验。患有院外心脏骤停后无 ST 段抬高的自主循环恢复的患者(年龄≥18 岁)由伦敦救护服务人员在心脏骤停现场通过安全的在线随机化系统随机分配(1:1)至七个心脏骤停中心之一的心脏导管实验室进行紧急分娩,或在英国伦敦的 32 家医院之一的地理上最近的急诊科进行标准护理。无法对提供干预措施的救护人员进行掩蔽,也无法对在医院报告治疗结果的人员进行掩蔽。主要结局是 30 天时的全因死亡率,在排除死亡率状态未知的患者后,按意向治疗人群(ITT)进行分析。安全性结局在 ITT 人群中进行分析。该试验在国际标准随机对照试验注册处(International Standard Randomised Controlled Trials Registry)进行了前瞻性注册,注册号为 96585404。
在 2018 年 1 月 15 日至 2022 年 12 月 1 日期间,纳入了 862 名患者,其中 431 名(50%)被随机分配至心脏骤停中心,431 名(50%)分配至标准护理组。20 名参与者退出了心脏骤停中心组,19 名退出了标准护理组,原因是缺乏同意或死亡率状态未知,因此,心脏骤停中心组有 411 名参与者,标准护理组有 412 名参与者进行主要分析。在可获得数据的 822 名参与者中,560 名(68%)为男性,262 名(32%)为女性。心脏骤停中心组有 258 名(63%)和标准护理组有 258 名(63%)参与者发生了 30 天死亡率的主要终点(校正后生存风险比为 1.00,95%CI 0.90-1.11;p=0.96)。心脏骤停中心组有 414 名患者中的 8 名(2%)和标准护理组有 413 名患者中的 3 名(1%)发生了严重不良事件,但均与试验干预无关。
在无 ST 段抬高的成年患者中,社区复苏后将患者送往心脏骤停中心并未降低死亡率。
英国心脏基金会。