Wong Li Siang, St George Jerome, Agyemang Kevin, Grivas Athanasios, Houston Deborah, Foo Sin Yee, Mullan Thomas
General Medicine, Royal Alexandra Hospital, Paisley, GBR.
Neurosurgery, Queen Elizabeth University Hospital, Glasgow, GBR.
Cureus. 2023 Jul 30;15(7):e42695. doi: 10.7759/cureus.42695. eCollection 2023 Jul.
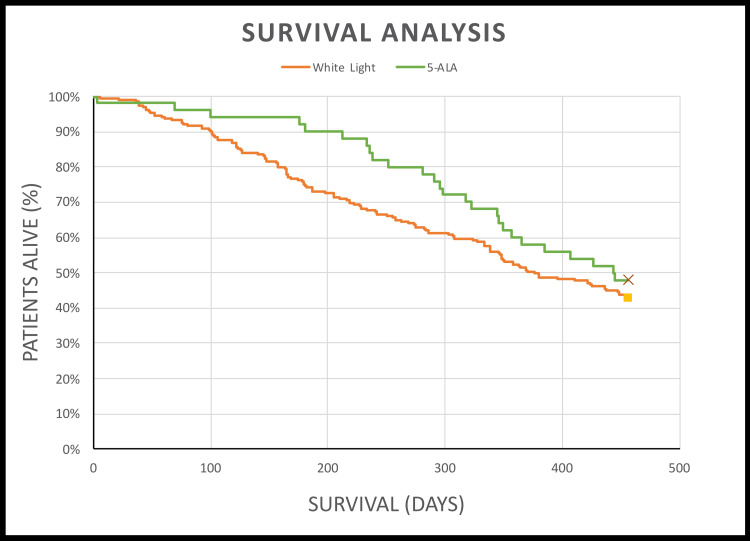
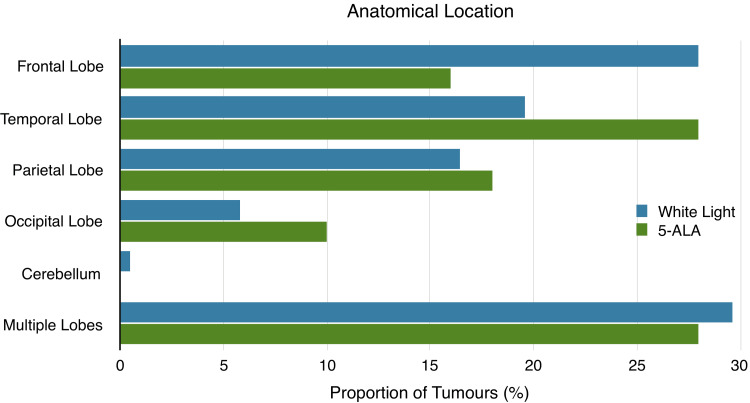
Background Glioblastoma (GBM) is the most common malignant primary brain tumour and confers a very poor prognosis. Maximal safe resection of tumour is the goal of neurosurgical intervention and may be more easily achieved through the use of surgical adjuncts such as fluorescence-guided surgery (FGS). 5-Aminolevulinic acid (5-ALA) accumulates in GBM tissue and fluoresce red, distinguishing tumour cells from the surrounding tissue and therefore making resection easier. 5-ALA-guided resection in GBM has been shown to increase resection rates and prolong progression-free survival without impacting post-operative morbidity. Radiotherapy and concomitant chemotherapy also improve survival in GBM. Other factors such as patient age and molecular status of the tumour also impact prognosis. Aims The aim of this study was to compare the outcomes of 5-ALA vs white light-guided resection for glioblastoma in the west of Scotland. Methods This was a retrospective analysis of baseline characteristics (age, sex, tumour molecular markers, radiotherapy, chemotherapy, anatomical location of tumour and treatment group) and outcomes (mortality, survival, degree of resection and performance status) of 239 patients who underwent primary resection of glioblastoma over a four-year period (2017-2020). A variety of statistical methods were used to analyse the relationship between each variable and surgical technique; multivariate Cox regression and the Kaplan-Meier method were used in survival analysis. Results 5-ALA-guided resection substantially improved resection rates (74.0% vs 40.2%). Mortality at 15 months was 5.1% lower in the 5-ALA group (52.0% vs 57.1%, p = 0.53), and patients lived an average of 68 days longer compared to the white light group (444 days vs 376 days, p = 0.21). There were negligible differences between treatment groups in terms of post-operative performance status (PS) and post-operative complications. In our multivariate Cox regression model, six factors were statistically significant at a level of p ≤ 0.05: age, radiotherapy, chemotherapy, O(6)-methylguanine-DNA methyltransferase (MGMT) methylation, anatomical location and >90% resection. Receiving chemotherapy and radiotherapy, MGMT methylation and undergoing >90% resection conferred a survival benefit at 15 months. Older age and multi-focal disease were related to a worsened mortality rate. Undergoing radiotherapy and maximal resection were the two greatest predictors of improved survival, reducing mortality risk by 58% and 51%, respectively. Conclusion 5-ALA-guided resection improved resection rates without impacting post-operative morbidity. 5-ALA-guided resection was associated with improved survival and lower mortality rate, but this was not statistically significant. Receiving chemoradiotherapy, MGMT methylation and undergoing maximal resection conferred a survival benefit, whilst older age and multi-focal disease were associated with a poorer prognosis.
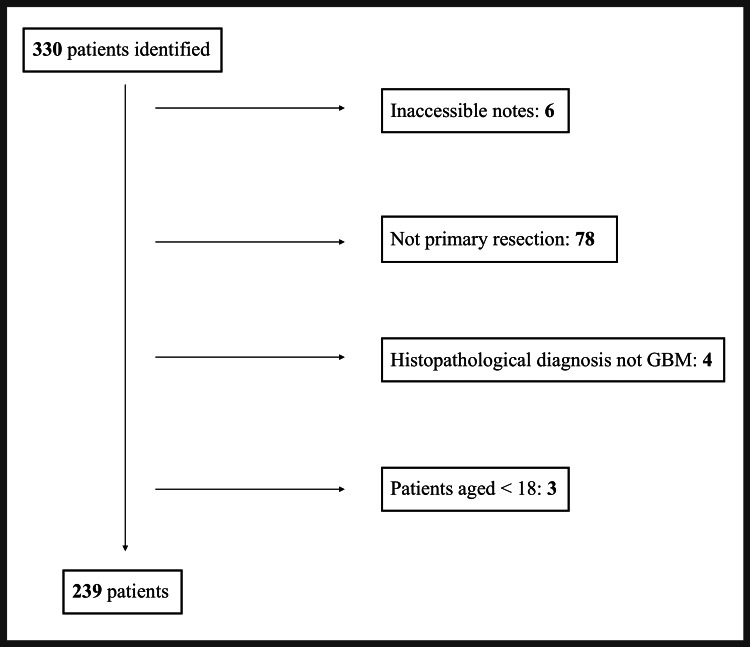
胶质母细胞瘤(GBM)是最常见的原发性恶性脑肿瘤,预后极差。肿瘤的最大安全切除是神经外科干预的目标,通过使用荧光引导手术(FGS)等手术辅助手段可能更容易实现。5-氨基酮戊酸(5-ALA)在GBM组织中蓄积并发出红色荧光,将肿瘤细胞与周围组织区分开来,从而使切除更容易。已证明5-ALA引导下的GBM切除术可提高切除率并延长无进展生存期,且不影响术后发病率。放疗和同步化疗也可改善GBM患者的生存期。其他因素,如患者年龄和肿瘤的分子状态,也会影响预后。目的:本研究旨在比较5-ALA引导与白光引导下切除苏格兰西部胶质母细胞瘤的疗效。方法:这是一项对239例在四年期间(2017 - 2020年)接受胶质母细胞瘤初次切除的患者的基线特征(年龄、性别、肿瘤分子标志物、放疗、化疗、肿瘤的解剖位置和治疗组)及疗效(死亡率、生存期、切除程度和功能状态)进行的回顾性分析。使用多种统计方法分析每个变量与手术技术之间的关系;生存分析采用多变量Cox回归和Kaplan-Meier方法。结果:5-ALA引导下的切除术显著提高了切除率(74.0%对40.2%)。5-ALA组15个月时的死亡率比白光组低5.1%(52.0%对57.1%,p = 0.53),且患者的平均生存期比白光组长68天(444天对376天,p = 0.21)。治疗组在术后功能状态(PS)和术后并发症方面差异可忽略不计。在我们的多变量Cox回归模型中,六个因素在p≤0.05水平上具有统计学意义:年龄、放疗、化疗、O(6)-甲基鸟嘌呤-DNA甲基转移酶(MGMT)甲基化、解剖位置和切除率>90%。接受化疗和放疗、MGMT甲基化以及切除率>90%在15个月时具有生存获益。年龄较大和多灶性疾病与死亡率恶化相关。接受放疗和最大程度切除是生存期改善的两个最大预测因素,分别将死亡风险降低58%和51%。结论:5-ALA引导下的切除术提高了切除率,且不影响术后发病率。5-ALA引导下的切除术与生存期改善和死亡率降低相关,但无统计学意义。接受放化疗、MGMT甲基化以及进行最大程度切除具有生存获益,而年龄较大和多灶性疾病与预后较差相关。