Department of Medicine, Division of General Internal Medicine, University of California, San Francisco (UCSF), San Francisco, CA, USA.
Multi-Ethnic Health Equity Research Center, UCSF, San Francisco, CA, USA.
J Gen Intern Med. 2023 Nov;38(14):3115-3122. doi: 10.1007/s11606-023-08189-1. Epub 2023 Aug 31.
Lung cancer screening (LCS) is recommended for individuals at high risk due to age and smoking history after a shared decision-making conversation. However, little is known about best strategies for incorporating shared decision-making, especially in a busy primary care setting.
To develop a novel tool, Lung Cancer Assessment of Risk and Education (LungCARE) to guide LCS decisions among eligible primary care patients.
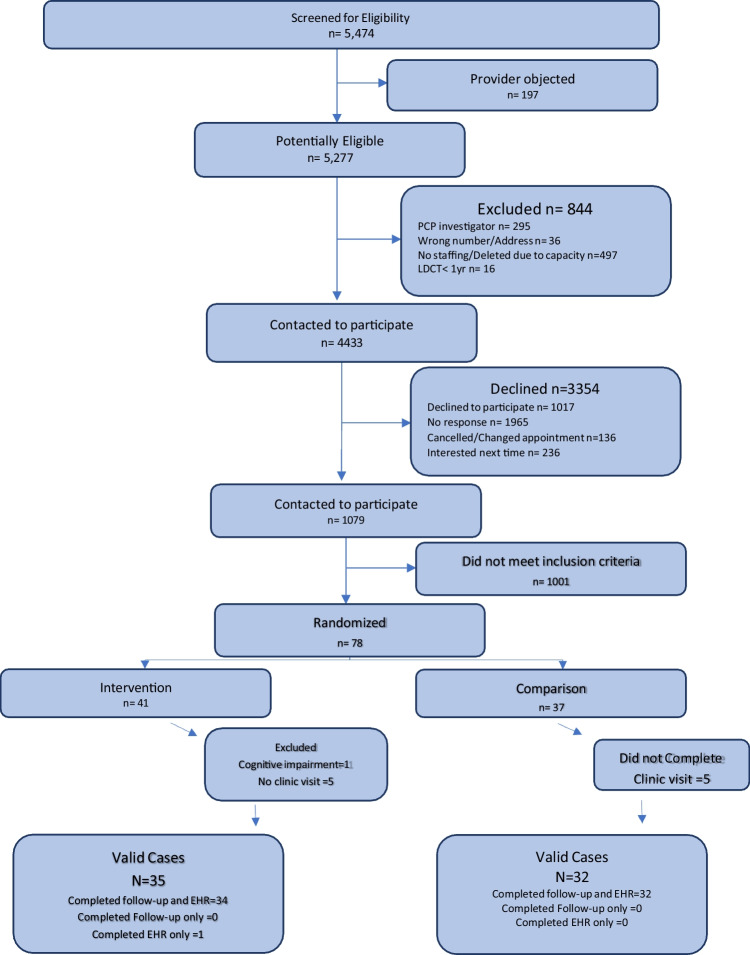
Pilot cluster randomized controlled trial of LungCARE versus usual care.
Patients of providers in a university primary care clinic, who met criteria for LCS.
Providers were randomized to LungCARE intervention or control. LungCARE participants completed a computer tablet-based video assessment of lung cancer educational needs in the waiting room prior to a primary care visit. Patient and provider both received a summary handout of patient concerns and responses.
All eligible patients completed baseline interviews by telephone. One week after the index visit, participants completed a follow-up telephone survey that assessed patient-physician discussion of LCS, referral to and scheduling of LCS, as well as LCS knowledge and acceptability of LungCARE. Two months after index visit, we reviewed patients' electronic health records (EHRs) for evidence of a shared decision-making conversation and referral to and receipt of LCS.
A total of 66 participants completed baseline and follow-up visits (34: LungCARE; 32: usual care). Mean age was 65.9 (± 6.0). Based on EHR review, compared to usual care, LungCARE participants were more likely to have discussed LCS with their physicians (56% vs 25%; p = 0.04) and to be referred to LCS (44% vs 13%; p < 0.02). Intervention participants were also more likely to complete LCS (32% vs 13%; p < 0.01) and had higher knowledge scores (mean score 6.5 (± 1.7) vs 5.5 (± 1.4; p < 0.01).
LungCARE increased discussion, referral, and completion of LCS and improved LCS knowledge.
NCT03862001.
肺癌筛查(LCS)建议在经过共同决策对话后,根据年龄和吸烟史,对高危人群进行。然而,对于最佳的共同决策实施策略,尤其是在繁忙的初级保健环境中,人们知之甚少。
开发一种新的工具,即肺癌风险评估和教育工具(LungCARE),以指导符合条件的初级保健患者进行 LCS 决策。
LungCARE 与常规护理的试点集群随机对照试验。
在一所大学初级保健诊所就诊的符合 LCS 标准的医生的患者。
医生被随机分配到 LungCARE 干预组或对照组。LungCARE 参与者在进行初级保健就诊前,在等候室完成基于计算机平板电脑的肺癌教育需求视频评估。患者和医生都收到了一份患者关注问题和答复的摘要单。
所有符合条件的患者均通过电话完成基线访谈。在指数就诊后的一周,参与者通过电话完成了一项随访调查,评估了患者与医生之间关于 LCS 的讨论、转诊和安排 LCS 的情况,以及 LCS 知识和对 LungCARE 的接受程度。在指数就诊后的两个月,我们查阅了患者的电子健康记录(EHR),以评估是否有共同决策对话以及是否转诊和接受 LCS。
共有 66 名参与者完成了基线和随访访问(34 名:LungCARE;32 名:常规护理)。平均年龄为 65.9(±6.0)岁。基于 EHR 审查,与常规护理相比,LungCARE 组的患者更有可能与他们的医生讨论 LCS(56%比 25%;p=0.04),并且更有可能被转诊接受 LCS(44%比 13%;p<0.02)。干预组也更有可能完成 LCS(32%比 13%;p<0.01),并且 LCS 知识得分更高(平均得分为 6.5(±1.7)比 5.5(±1.4;p<0.01)。
LungCARE 增加了 LCS 的讨论、转诊和完成率,并提高了 LCS 知识。
NCT03862001。