Institute of Clinical Pathology, Kepler University Hospital, Krankenhausstr. 9, 4021, Linz, Austria.
Medical Faculty, Johannes Kepler University, Linz, Austria.
Virchows Arch. 2023 Nov;483(5):611-619. doi: 10.1007/s00428-023-03622-6. Epub 2023 Sep 1.
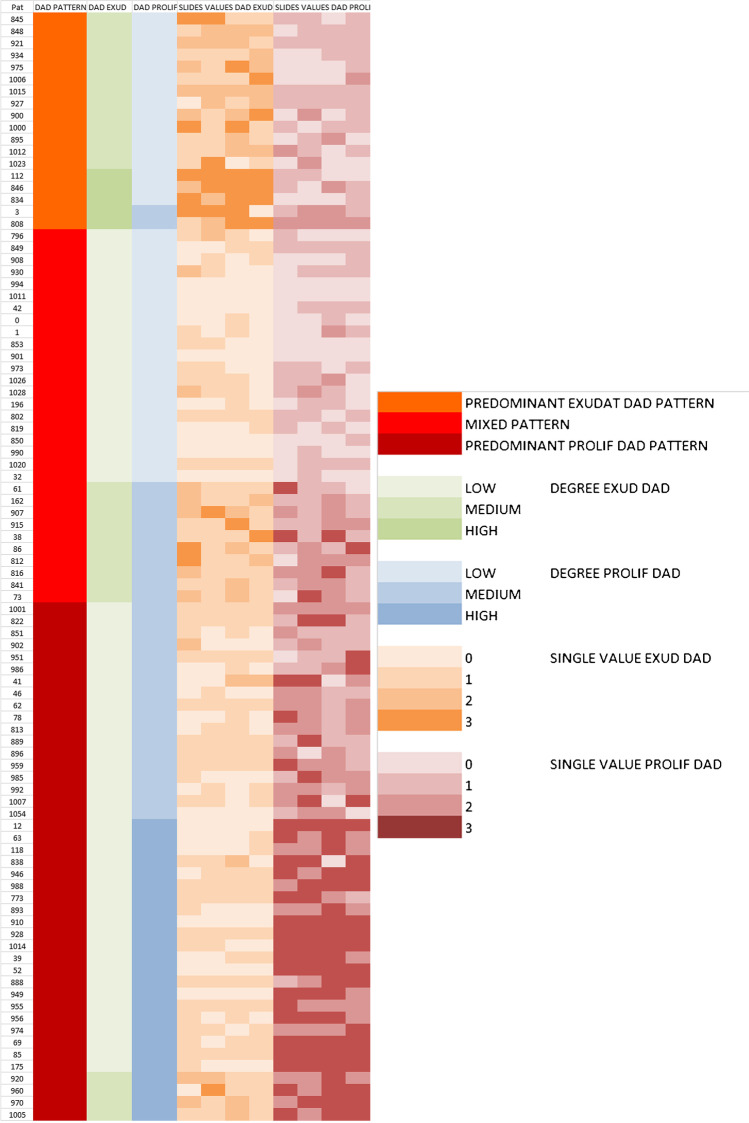
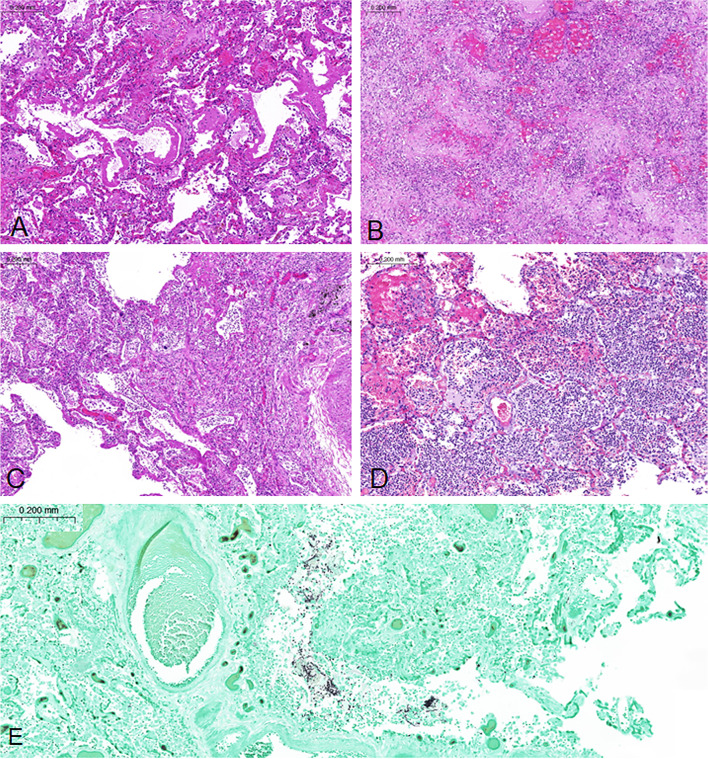
Minimally invasive autopsies (MIAs) allow the collection of tissue samples for diagnostic and research purposes in special situations, e.g., when there is a high risk of infection which is the case in the context of COVID-19 or restrictions due to legal or personal reasons. We performed MIA to analyze lung tissue from 92 COVID-19 patients (mean age 78 years; range 48-98; 35 women, 57 men), representing 44% of all patients who died from the disease between October 2020 and April 2021. An intercostal approach was used with removal of a 5-cm rib section followed by manual collection of four lung tissue samples (5-8 cm in size). Diffuse alveolar damage (DAD) was found in 89 (97%) patients at various stages. Exudative DAD (eDAD) predominated in 18 (20%) patients, proliferative DAD (pDAD) in 43 (47%) patients, and mixed DAD (mDAD) in 31 (34%) patients. There were no significant differences in the predominant DAD pattern between tissue samples from the same patient. Additional purulent components were present in 46 (50%) cases. Fungi were detected in 11 (12%) patients. The pDAD pattern was associated with longer hospital stay including intensive care unit (p=0.026 and p<0.001) and younger age (p=0.019). Positive bronchoalveolar lavage and blood cultures were observed more frequently in pDAD patterns (p<0.001; p=0.018). In contrast, there was no significant association between intravital positive microbiological results and superimposed bronchopneumonia or fungal infection at autopsy. Having demonstrated the characteristic lung changes in a large longitudinal autopsy series, we conclude that the presented MIA approach can be considered a reliable and safe method for performing post mortem lung diagnostics in COVID-19 and other high-risk situations. The lack of correlation between histological changes indicative of bacterial or fungal superinfection and microbiology could have clinical implications for disease and treatment surveillance.
微创解剖(MIA)允许在特殊情况下收集组织样本用于诊断和研究目的,例如在存在高感染风险的情况下,例如在 COVID-19 或由于法律或个人原因而受到限制的情况下。我们对 92 例 COVID-19 患者(平均年龄 78 岁;范围 48-98;35 名女性,57 名男性)的肺组织进行了 MIA,这些患者代表了 2020 年 10 月至 2021 年 4 月期间死于该病的所有患者的 44%。采用肋间入路切除 5cm 肋骨段,然后手动采集 4 个肺组织样本(大小为 5-8cm)。在不同阶段发现 89 例(97%)患者存在弥漫性肺泡损伤(DAD)。渗出性 DAD(eDAD)在 18 例(20%)患者中占优势,增殖性 DAD(pDAD)在 43 例(47%)患者中占优势,混合性 DAD(mDAD)在 31 例(34%)患者中占优势。同一患者的组织样本中,主要 DAD 模式无显著差异。46 例(50%)患者存在化脓性成分。11 例(12%)患者检测到真菌。pDAD 模式与更长的住院时间包括重症监护病房(p=0.026 和 p<0.001)和更年轻的年龄(p=0.019)相关。pDAD 模式中更频繁观察到阳性支气管肺泡灌洗和血液培养(p<0.001;p=0.018)。相比之下,在活体内微生物学阳性结果与尸检时合并支气管肺炎或真菌感染之间无显著相关性。在大型纵向尸检系列中证明了特征性的肺部变化,我们得出结论,所提出的 MIA 方法可被视为在 COVID-19 和其他高危情况下进行死后肺诊断的可靠和安全方法。组织学变化表明细菌或真菌感染的缺乏与微生物学之间的相关性可能对疾病和治疗监测具有临床意义。