Ganokroj Phob, Fossum Bradley W, Hollenbeck Justin, Whalen Ryan J, Garcia Alexander R, Foster Michael J, Provencher Capt Matthew T
Steadman Philippon Research Institute, Vail, Colorado, USA.
Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand.
Orthop J Sports Med. 2023 Aug 22;11(8):23259671231182978. doi: 10.1177/23259671231182978. eCollection 2023 Aug.
Segmental medial meniscal allograft transplantation (MAT) has been shown to restore knee biomechanics; however, stable fixation of the transplantation is critical to avoid extrusion and maximize healing.
To evaluate the degree of meniscal extrusion and biomechanical function of segmental medial MAT performed with meniscocapsular sutures versus repair augmentation with knotless suture anchors.
Controlled laboratory study.
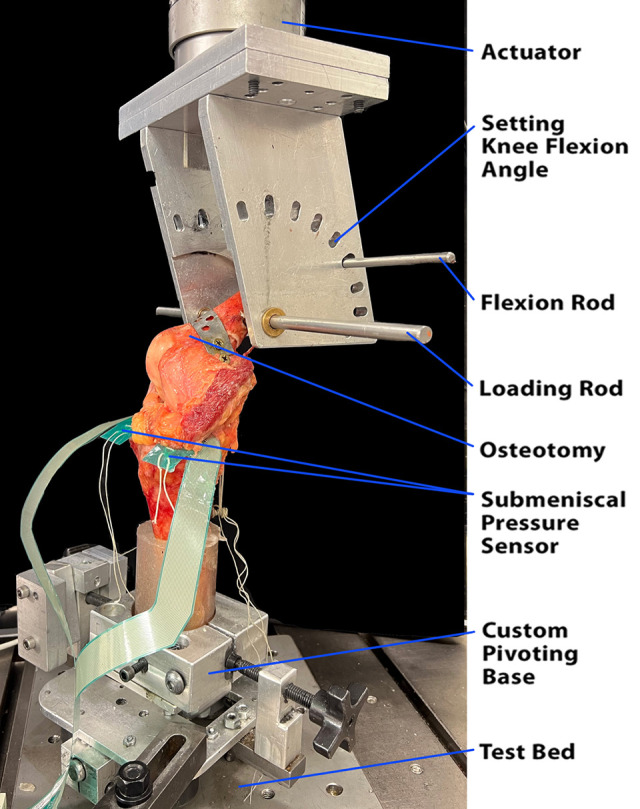
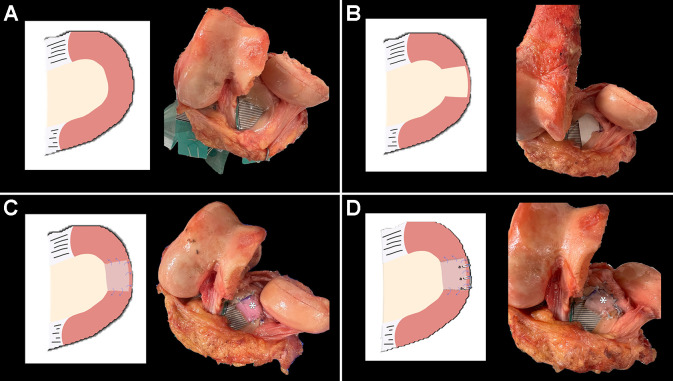
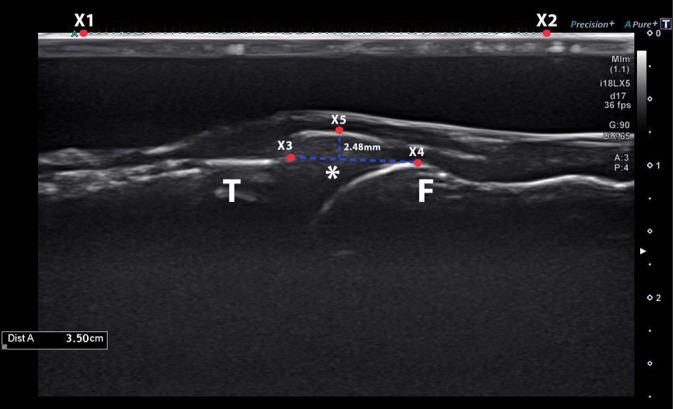
Segmental midbody medial meniscectomy and subsequent segmental medial MAT were performed on 10 fresh-frozen cadaveric knees. The knees were then loaded in a dynamic tensile testing machine to 1000 N for 60 seconds at 0°, 30°, 60°, and 90° of flexion, and 4 conditions were tested: (1) intact, (2) segmental defect, (3) inside-out segmental repair, and (4) anchor plus inside-out segmental repair of the medial MAT. Meniscal extrusion was measured using high-fidelity ultrasound imaging. The mean contact area and the mean and peak contact pressures were assessed with submeniscal pressure-mapping sensors. Data from testing conditions were compared with 2-way repeated-measures analysis of variance, with pairwise comparison using the Bonferroni method.
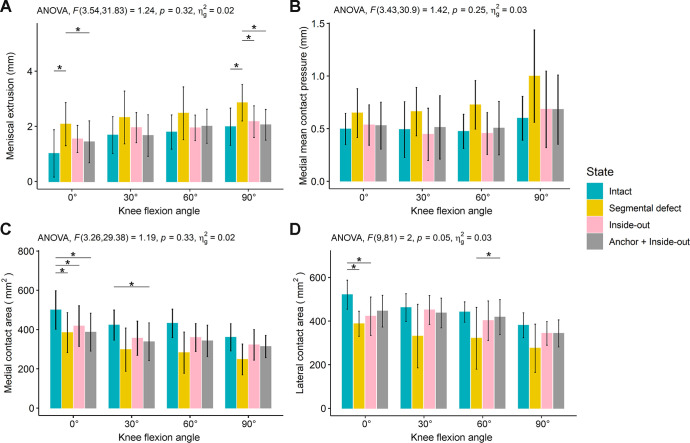
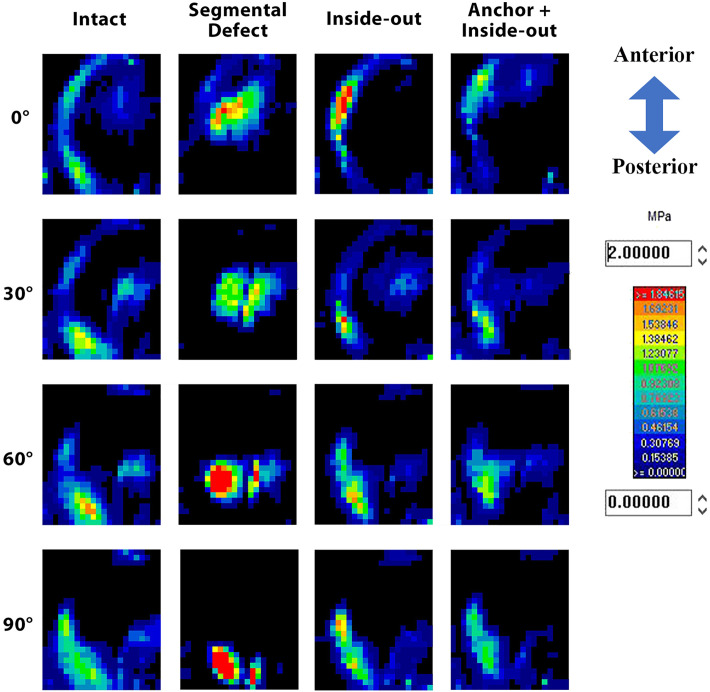
At 90° of flexion, the segmental defect state showed a higher degree of meniscal extrusion compared with all other states ( ≤ .012). There was no difference in the degree of meniscal extrusion between the intact state and the inside-out repair or anchor plus inside-out segmental repair states at all knee flexion angles ( > .05). There was no significant difference in the mean and peak contact pressures among the 4 states at all flexion angles except that at 0° of knee flexion there was significantly lower peak contact pressure at the medial compartment after anchor plus inside-out segmental repair compared with the segmental defect state ( = .048).
Meniscal extrusion was not significantly increased at any flexion angle after segmental resection. The addition of knotless anchors did not improve meniscal extrusion or contact pressures/area compared with capsular repair alone. The addition of knotless anchors did improve contact mechanics from the segmental defect state, but only at 0° of flexion.
The addition of knotless suture anchors to segmental meniscal transplantation increased stabilization of the meniscus at full extension compared with repair with sutures alone. This increased stabilization may lead to better long-term outcomes.
节段性内侧半月板同种异体移植(MAT)已被证明可恢复膝关节生物力学;然而,移植的稳定固定对于避免半月板挤出并使愈合最大化至关重要。
评估采用半月板-关节囊缝合与使用无结缝合锚钉进行修复增强的节段性内侧MAT的半月板挤出程度和生物力学功能。
对照实验室研究。
对10个新鲜冷冻尸体膝关节进行节段性半月板体部内侧切除术及随后的节段性内侧MAT。然后将膝关节置于动态拉伸试验机中,在0°、30°、60°和90°屈曲位施加1000 N的力,持续60秒,并测试4种情况:(1)完整状态;(2)节段性缺损状态;(3)由内向外节段性修复状态;(4)内侧MAT的锚钉加由内向外节段性修复状态。使用高保真超声成像测量半月板挤出情况。使用半月板下压力映射传感器评估平均接触面积、平均接触压力和峰值接触压力。对测试情况的数据进行双向重复测量方差分析,并使用Bonferroni方法进行两两比较。
在90°屈曲位时,节段性缺损状态与所有其他状态相比,半月板挤出程度更高(P≤0.012)。在所有膝关节屈曲角度下,完整状态与由内向外修复状态或锚钉加由内向外节段性修复状态之间的半月板挤出程度无差异(P>0.05)。在所有屈曲角度下,4种状态之间的平均接触压力和峰值接触压力均无显著差异,但在膝关节0°屈曲位时,锚钉加由内向外节段性修复后内侧间室的峰值接触压力显著低于节段性缺损状态(P = 0.048)。
节段性切除后,在任何屈曲角度下半月板挤出均未显著增加。与单纯关节囊修复相比,添加无结锚钉并未改善半月板挤出或接触压力/面积。添加无结锚钉确实改善了节段性缺损状态下的接触力学,但仅在0°屈曲位时。
与单纯缝合修复相比,在节段性半月板移植中添加无结缝合锚钉可增加半月板在完全伸展时的稳定性。这种增加的稳定性可能会带来更好的长期效果。