Department of Medical Surgical Sciences and Advanced Technologies "GF Ingrassia", University Hospital Policlinico "G. Rodolico-San Marco", Catania, Italy.
Radiology Unit 1, University Hospital Policlinico "G. Rodolico-San Marco", Catania, Italy.
Br J Radiol. 2023 Nov;96(1151):20221160. doi: 10.1259/bjr.20221160. Epub 2023 Oct 3.
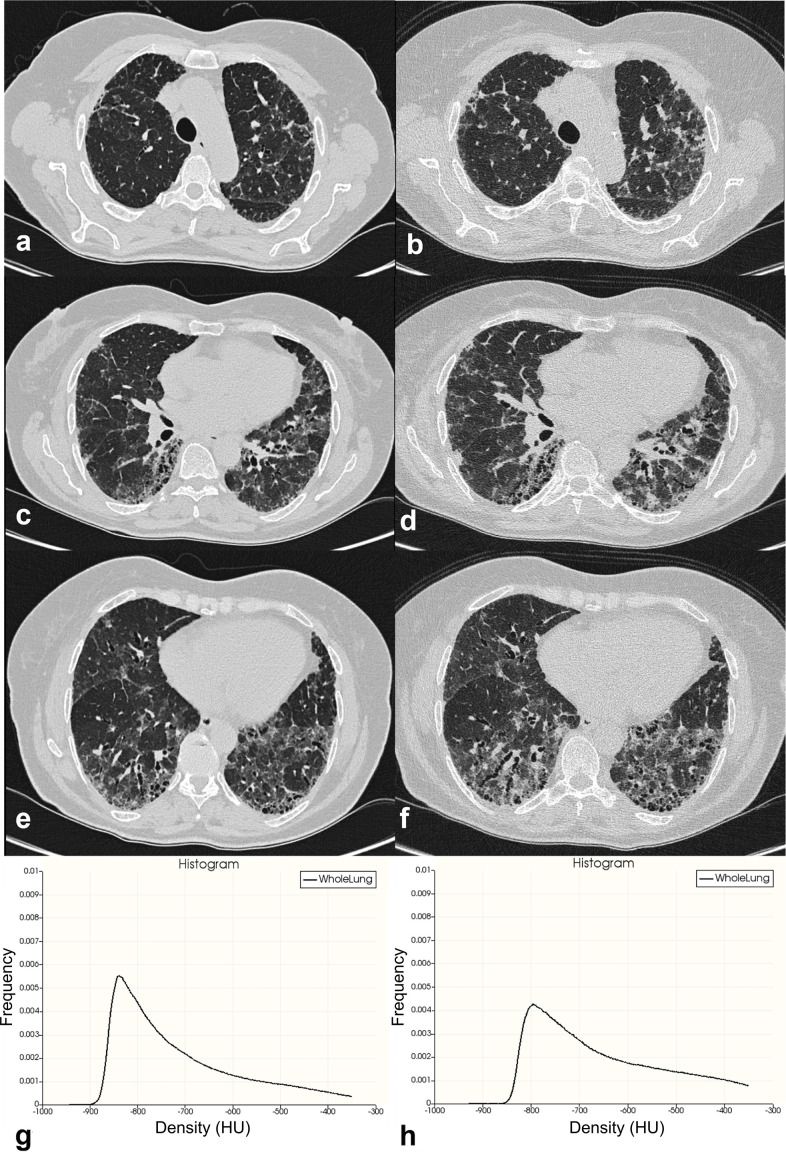
To investigate relationships between histogram-based high-resolution CT (HRCT) indexes and pulmonary function tests (PFTs) in interstitial lung diseases.
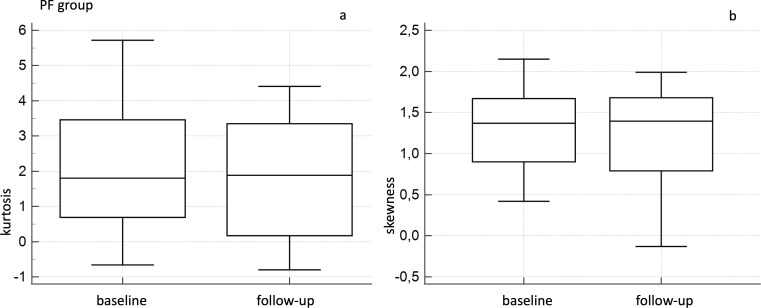
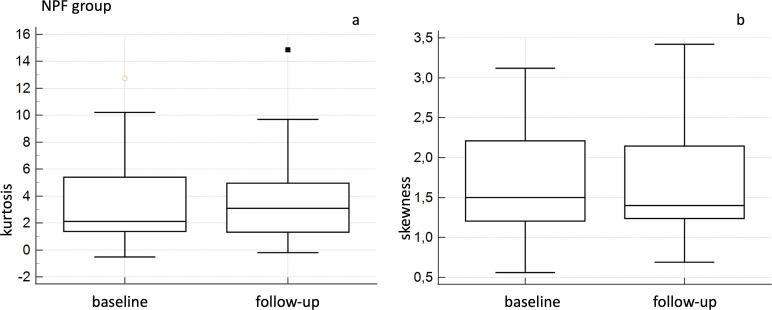
Forty-nine patients having baseline and 1-year HRCT examinations and PFTs were investigated. Histogram-based HRCT indexes were calculated; strength of associations with PFTs was investigated using Pearson correlation. Patients were divided into progressive and non-progressive groups. HRCT indexes were compared between the two groups using the -test; within each group, baseline and follow-up Wilcoxon analysis was performed. Receiver operating characteristic analysis was used for predicting disease progression.
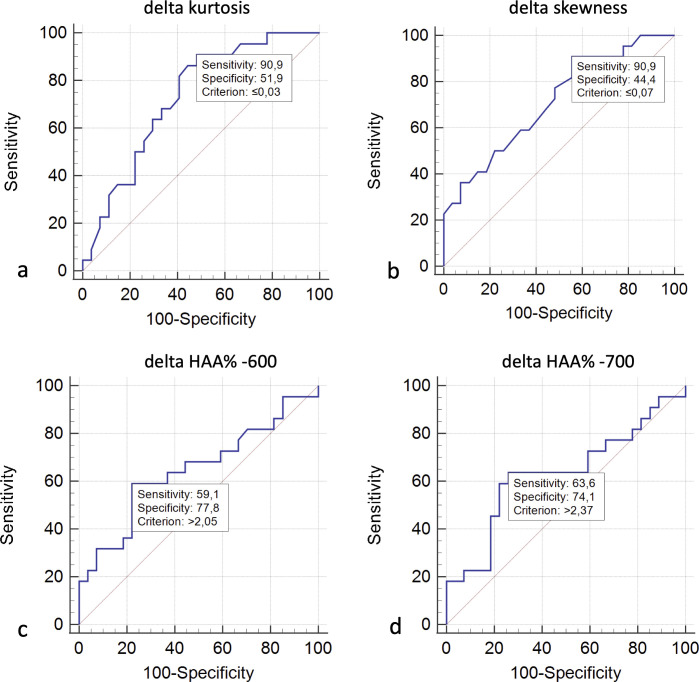
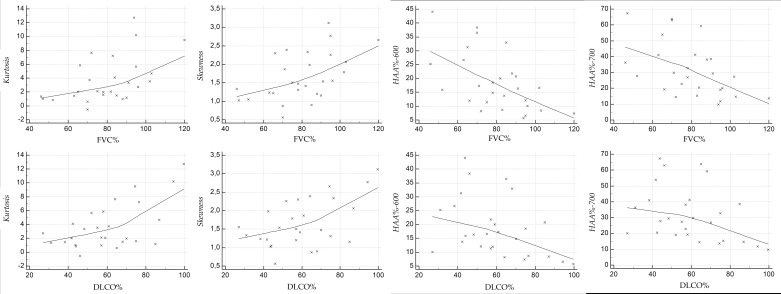
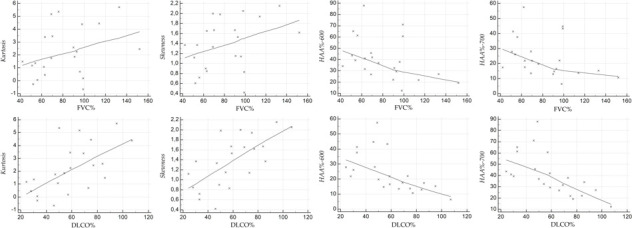
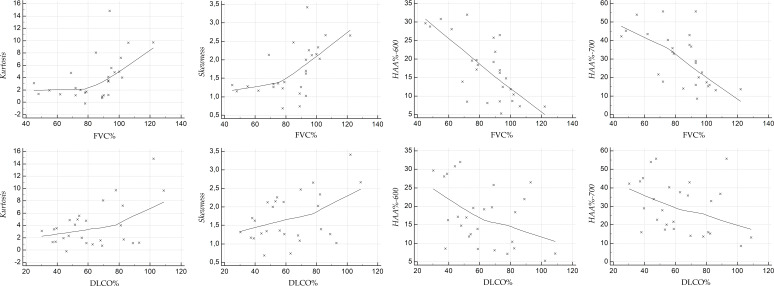
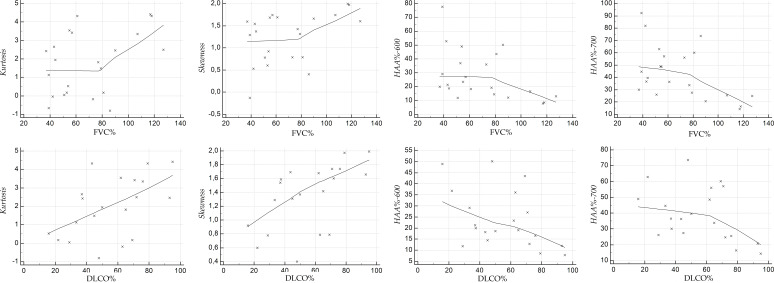
At baseline, moderate correlations were observed considering kurtosis and diffusion capacity of the lungs for carbon monoxide (DLCO) ( = 0.54) and skewness and DLCO ( = 0.559), whereas weak but significant correlations were observed between forced vital capacity and kurtosis ( = 0.368, = 0.009) and forced vital capacity and skewness ( = 0.391, = 0.005). Negative correlations were reported between HAA% and PFTs (from = -0.418 up to = -0.507). At follow-up correlations between quantitative indexes and PFTs were also moderate, except for high attenuation area (HAA)% -700 and DLCO ( = -0.397). In progressive subgroup, moderate and strong correlations were found between DLCO and HRCT indexes ( = 0.595 kurtosis, = 0.672 skewness, r=-0. 598 HAA% -600 and = -0.626 HAA% -700). At follow-up, we observed significant differences between the two groups for kurtosis ( = 0.029), HAA% -600 ( = 0.04) and HAA% -700 ( = 0.02). To predict progression, ROC analysis reported sensitivity of 90.9% and specificity of 51.9% using a threshold value of δ kurtosis <0.03.
At one year, moderate correlations suggest that progression could be assessed through HRCT quantification.
This study promotes histogram-based HRCT indexes in the assessment of progressive pulmonary fibrosis.
研究基于高分辨率 CT(HRCT)直方图的指标与肺间质疾病的肺功能检查(PFT)之间的关系。
对 49 例基线和 1 年 HRCT 检查及 PFT 患者进行调查。计算基于直方图的 HRCT 指标;采用 Pearson 相关分析探讨与 PFT 的关联强度。将患者分为进展组和非进展组。使用 t 检验比较两组之间的 HRCT 指标;在每组内进行基线和随访 Wilcoxon 分析。采用受试者工作特征分析(ROC)预测疾病进展。
在基线时,峰度和一氧化碳弥散量(DLCO)( = 0.54)以及偏度和 DLCO( = 0.559)之间观察到中度相关,而用力肺活量与峰度( = 0.368, = 0.009)和用力肺活量与偏度( = 0.391, = 0.005)之间存在弱但显著的相关性。HAA%与 PFT 之间存在负相关(从 = -0.418 到 = -0.507)。在随访时,除了高衰减区(HAA)% -700 和 DLCO 外,定量指标与 PFT 之间的相关性也呈中度( = -0.397)。在进展亚组中,DLCO 与 HRCT 指标之间存在中度和高度相关性( = 0.595 峰度, = 0.672 偏度,r=-0.598 HAA% -600, = -0.626 HAA% -700)。在随访时,我们观察到两组之间的峰度( = 0.029)、HAA% -600( = 0.04)和 HAA% -700( = 0.02)有显著差异。为了预测进展,ROC 分析报告使用阈值 δ 峰度 <0.03 时的敏感性为 90.9%,特异性为 51.9%。
在 1 年内,中度相关性表明可以通过 HRCT 定量评估进展。
本研究促进了基于直方图的 HRCT 指标在评估进行性肺纤维化中的应用。