CorEvitas LLC, Waltham, MA, USA.
Corrona Research Foundation, Albany, NY, USA.
Arthritis Res Ther. 2023 Sep 9;25(1):166. doi: 10.1186/s13075-023-03120-9.
Real-world studies assessing the comparative effectiveness of biologic or targeted synthetic disease-modifying antirheumatic drugs (b/tsDMARDs) as first-line targeted therapy are scarce. We analyzed the real-world persistence and effectiveness of etanercept (ETN), adalimumab (ADA), and Janus kinase inhibitors (JAKis) as first-line therapy in b/tsDMARD-naïve patients with rheumatoid arthritis (RA).
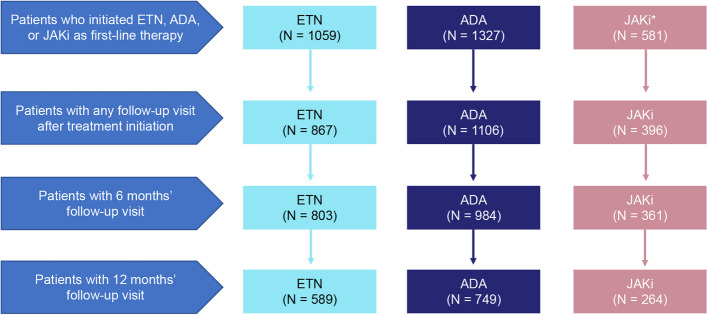
Adults (≥ 18 years) enrolled in the CorEvitas RA Registry and initiating ETN, ADA, or a JAKi (alone or in combination with csDMARDs) between November 2012 and June 2021 were included if they had 6 and/or 12 months' follow-up. Treatment persistence and effectiveness outcomes including the change in Clinical Disease Activity Index (CDAI) and patient-reported outcomes (PROs) were evaluated at follow-up, adjusting for covariates using linear and logistic regression models. An exploratory analysis for patients on monotherapy was also conducted.
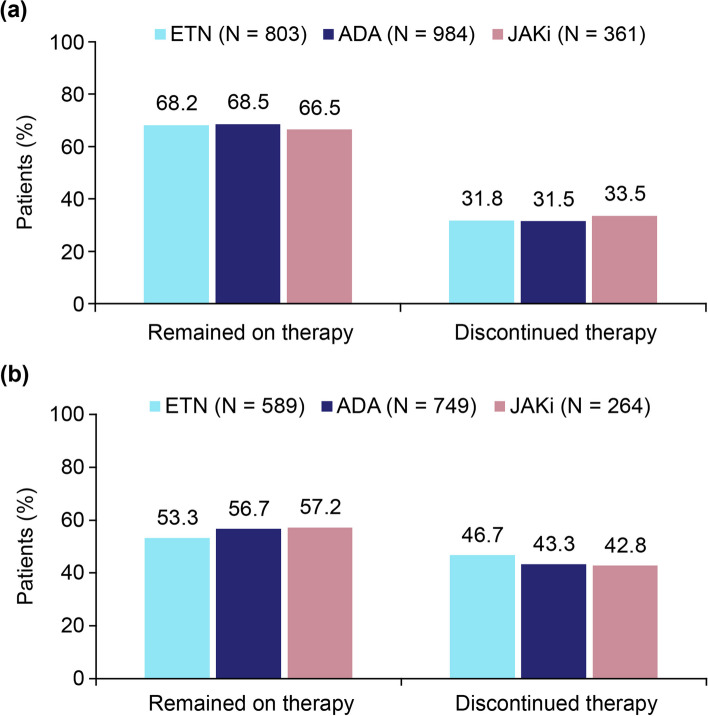
Of 1059 ETN, 1327 ADA, and 581 JAKi initiators; 803 ETN, 984 ADA, and 361 JAKi initiators had 6 months' follow-up. JAKi initiators were older and had a relatively longer disease duration than ETN or ADA initiators (mean age: 61.3 vs 54.5 and 55.5 years; mean duration of RA: 8.1 vs 5.7 and 5.6 years). Unadjusted mean improvements in CDAI and PROs were similar between the groups at 6 months, except the proportion achieving LDA, remission, and MCID in CDAI, which were numerically higher in the ETN and ADA groups vs JAKi group (LDA: 43.4% and 41.9% vs 32.5%; remission: 18.2% and 15.1% vs 11.5%; MCID: 46.5% and 47.8% vs 38.0%). Adjusted effectiveness results did not reveal statistically significant differences between treatment groups at 6 months, with an exception in MCID (odds ratio [95% CI] for JAKi vs ETN: 0.65 [0.43-0.98]). At 6 months, 68.2% of ETN, 68.5% of ADA, and 66.5% of JAKi initiators remained on therapy. The findings at 12 months' follow-up and sensitivity analysis among monotherapy initiators also showed no differences in effectiveness outcomes between the groups.
This analysis of real-world data from the CorEvitas RA Registry did not show differences in clinical effectiveness and treatment persistence rates in b/tsDMARD-naïve patients initiating ETN, ADA, or JAKi as first-line targeted therapy either alone or in combination with csDMARDs.
评估生物制剂或靶向合成疾病修饰抗风湿药物(b/tsDMARDs)作为一线靶向治疗的比较疗效的真实世界研究很少。我们分析了在生物制剂/靶向合成疾病修饰抗风湿药物初治的类风湿关节炎(RA)患者中,依那西普(ETN)、阿达木单抗(ADA)和 Janus 激酶抑制剂(JAKi)作为一线治疗的真实世界中的持续性和疗效。
2012 年 11 月至 2021 年 6 月期间,纳入在 CorEvitas RA 登记处登记并开始接受 ETN、ADA 或 JAKi(单独或与 csDMARDs 联合使用)治疗且有 6 个月和/或 12 个月随访的成年人(≥18 岁)。使用线性和逻辑回归模型,根据协变量调整,在随访时评估治疗持续性和疗效结果,包括临床疾病活动指数(CDAI)和患者报告的结果(PROs)的变化。还对接受单药治疗的患者进行了探索性分析。
纳入 1059 例 ETN、1327 例 ADA 和 581 例 JAKi 初治患者;803 例 ETN、984 例 ADA 和 361 例 JAKi 初治患者有 6 个月的随访。JAKi 初治者比 ETN 或 ADA 初治者年龄更大,疾病病程也更长(平均年龄:61.3 岁比 54.5 岁和 55.5 岁;平均 RA 病程:8.1 年比 5.7 年和 5.6 年)。6 个月时,各组之间的 CDAI 和 PROs 改善的未经调整的均值相似,但 CDAI 中达到低疾病活动度、缓解和 MCID 的比例,ETN 和 ADA 组高于 JAKi 组(低疾病活动度:43.4%和 41.9%比 32.5%;缓解:18.2%和 15.1%比 11.5%;MCID:46.5%和 47.8%比 38.0%)。6 个月时,调整后的疗效结果并未显示各组之间存在统计学上的显著差异,但 MCID 除外(JAKi 与 ETN 的比值比[95%CI]:0.65[0.43-0.98])。6 个月时,68.2%的 ETN、68.5%的 ADA 和 66.5%的 JAKi 初治者仍在接受治疗。12 个月随访和单药初治者的敏感性分析结果也显示,各组之间的疗效结果无差异。
这项来自 CorEvitas RA 登记处的真实世界数据分析并未显示,在生物制剂/靶向合成疾病修饰抗风湿药物初治的类风湿关节炎患者中,依那西普、阿达木单抗或 JAKi 作为一线靶向治疗,无论是单独使用还是与 csDMARDs 联合使用,在临床疗效和治疗持续率方面存在差异。