Wang Danfeng, Liao Chengyu, Tian Yifeng, Zheng Ting, Ye Huazhen, Yu Zenggui, Jiang Jundan, Su Jiawei, Chen Shi, Zheng Xiaochun
Shengli Clinical Medical College of Fujian Medical University, Fuzhou, China.
Department of Anesthesiology, Fujian Provincial Hospital, Fuzhou, China.
EClinicalMedicine. 2023 Aug 31;63:102188. doi: 10.1016/j.eclinm.2023.102188. eCollection 2023 Sep.
Convincing clinical evidence regarding completely opioid-free postoperative pain management using erector spinae plane block (ESPB) in patients undergoing open major hepatectomy (OMH) is lacking. Herein, we aimed to compare the postoperative analgesic efficacy of the visualised continuous opioid-free ESPB (VC-ESPB) and conventional intravenous opioid-based postoperative pain management in hepatocellular carcinoma (HCC) patients undergoing OMH.
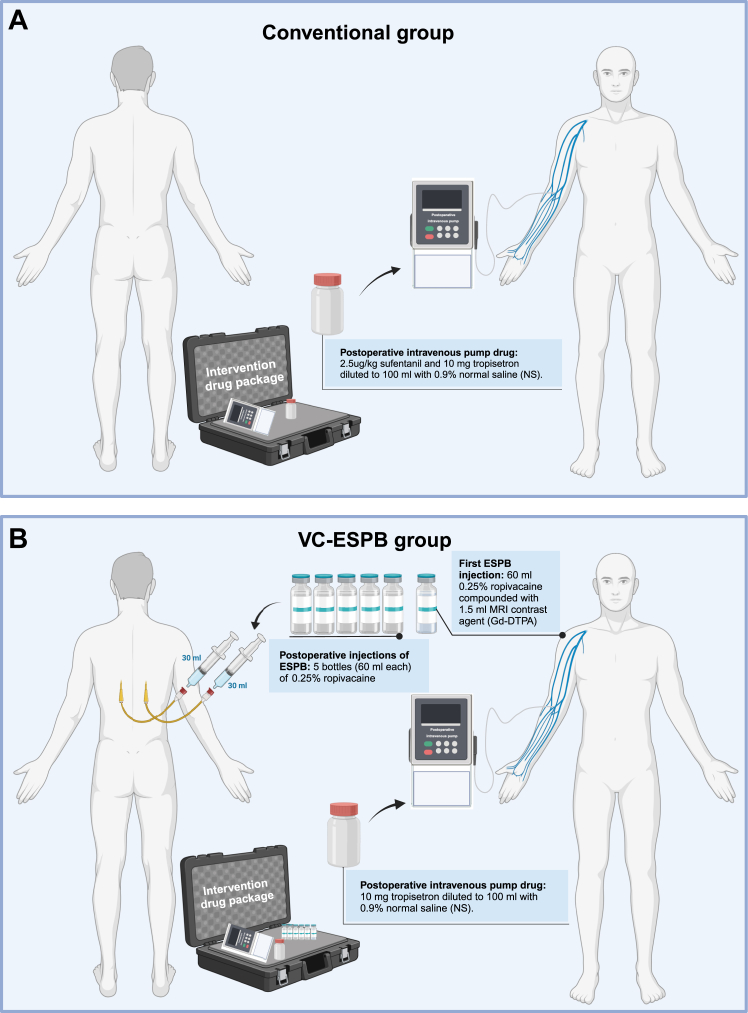
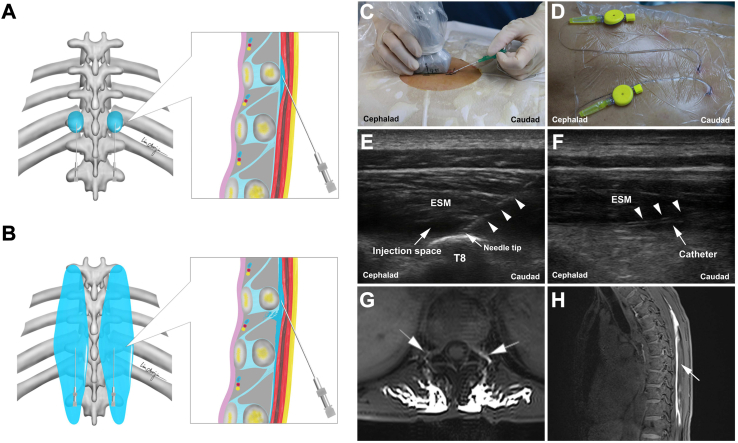
This open-label, randomised, controlled, non-inferiority trial enrolled patients with HCC undergone open major hepatectomy in Fujian Provincial Hospital and compared the postoperative analgesic efficacy of VC-ESPB (VC-ESPB group) and conventional intravenous opioid-based pain management regimen (conventional group). Patients were randomly assigned (1:1) to VC-ESPB group and conventional group. Patients were not masked to treatment allocation. The VC-ESPB group was treated with intermittent injections of 0.25% ropivacaine (bilateral, 30 mL each side) given every 12 h through catheters placed in the space of erector spinae and an opioid-free intravenous pump (10-mg tropisetron diluted to 100 mL with 0.9% normal saline [NS]) for postoperative pain management. The conventional group did not receive ESPB and was treated with a conventional intravenous opioid-based pump (2.5-μg/kg sufentanil and 10-mg tropisetron diluted to 100 mL with 0.9% NS). Patients in the VC-ESPB group underwent magnetic resonance imaging (MRI) to identify local anaesthetic diffusion after ESPB was performed under ultrasound guidance. The primary outcome was postoperative analgesic efficacy, which was indicated by the cumulative area under the curve (AUC) of the pain visual analogue scale scores (range, 0-10; a higher score indicates more pain) obtained at rest and at movement until 48 h postoperatively after leaving the post-anaesthesia care unit (PACU). Herein, an AUC of 26.5 was set as the noninferiority margin, which needed to be satisfied for both cumulative AUC at rest and cumulative AUC at movement. Per protocol participants were included in primary and safety analyses. This trial was registered with ChiCTR.org.cn (ChiCTR1900026583).
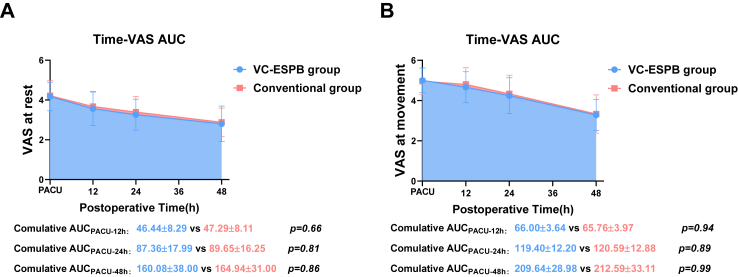
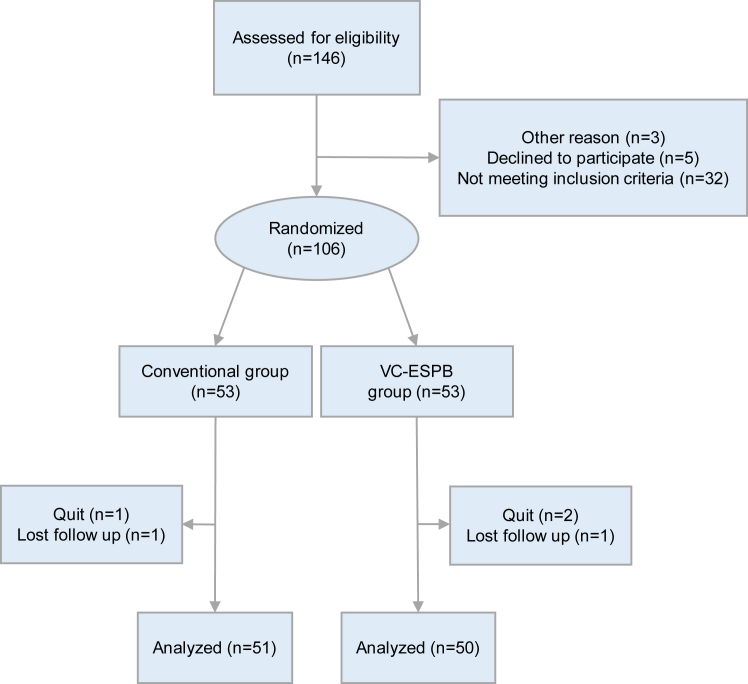
Between October 30, 2019, and May 1, 2023, 106 patients were enrolled and randomly assigned to the VC-ESPB group (n = 53) and the conventional group (n = 53). After the dropout (n = 5), a total of 101 patients (VC-ESPB group, n = 50; conventional group, n = 51) were analysed. Both the level of cumulative AUC (at rest: 160.08 ± 38.00 164.94 ± 31.00; difference [90% CI], -4.861 [-16.308, 6.585]) and cumulative AUC (at movement: 209.64 ± 28.98 212.59 ± 33.11; difference [90% CI], -2.948 [-13.236, 7.339]) were similar between the VC-ESPB and control groups within the first postoperative 48 h. The upper limit of the 90% CIs for the difference in cumulative ACUP at rest and at movement did not reach the upper inferiority margin (26.5). During the first postoperative 48 h, the rate of nonsteroidal anti-inflammatory drug rescue analgesia was similar between the VC-ESPB group and conventional group (n = 16, 32.0% n = 11, 21.6%; = 0.236). Treatment-related death was not observed in the VC-ESPB group (n = 0, 0%) and conventional group (n = 0, 0%). In VC-ESPB group, local site paralysis (n = 1, 2.0%) was observed in one patient and rash (n = 1, 2.0%) was observed in another patient. One patient in the conventional group was observed with rash preoperatively (n = 1, 2.0%). The VC-ESPB group had significantly lower rates of postoperative nausea (n = 2, 4.0%, n = 9, 17.6%, = 0.028), vomiting (n = 1, 2.0% n = 8, 15.7%, = 0.031) and lower incidence of major complications (n = 4, 8.0% n = 6, 11.8%; = 0.033).
This study demonstrates the noninferiority of VC-ESPB when compared with the conventional opioid-based approach for postoperative pain management after OMH, suggesting that it is feasible to achieve opioid-free postoperative pain management for OMH.
The Joint Funds for the Innovation of Science and Technology, Fujian Province, China; the Youth Scientific Research Project of Fujian Provincial Health Commission; the Fujian Research and Training Grants for Young and Middle-aged Leaders in Healthcare; and the Key Clinical Specialty Discipline Construction Program of Fujian, China.
对于接受开放性大肝切除术(OMH)的患者,使用竖脊肌平面阻滞(ESPB)进行完全无阿片类药物的术后疼痛管理,目前缺乏令人信服的临床证据。在此,我们旨在比较可视化连续无阿片类药物ESPB(VC-ESPB)与传统静脉注射阿片类药物术后疼痛管理在接受OMH的肝细胞癌(HCC)患者中的术后镇痛效果。
本开放标签、随机、对照、非劣效性试验纳入了在福建省立医院接受开放性大肝切除术的HCC患者,比较了VC-ESPB(VC-ESPB组)和传统静脉注射阿片类药物疼痛管理方案(传统组)的术后镇痛效果。患者被随机分配(1:1)至VC-ESPB组和传统组。患者不设治疗分配盲法。VC-ESPB组通过置于竖脊肌间隙的导管每12小时间歇性注射0.25%罗哌卡因(双侧,每侧30 mL),并使用无阿片类药物静脉泵(10 mg托烷司琼用0.9%生理盐水[NS]稀释至100 mL)进行术后疼痛管理。传统组未接受ESPB,采用传统静脉注射阿片类药物泵(2.5 μg/kg舒芬太尼和10 mg托烷司琼用0.9% NS稀释至100 mL)治疗。VC-ESPB组患者在超声引导下进行ESPB后接受磁共振成像(MRI)以确定局部麻醉药的扩散情况。主要结局是术后镇痛效果,通过离开麻醉后护理单元(PACU)后至术后48小时静息和活动时获得的疼痛视觉模拟量表评分(范围0-10;分数越高疼痛越剧烈)的曲线下面积(AUC)累积值来表示。在此,将AUC 26.5设定为非劣效性界值,静息和活动时的累积AUC均需满足该界值。符合方案的参与者纳入主要和安全性分析。本试验在ChiCTR.org.cn注册(ChiCTR1900026583)。
在2019年10月30日至2023年5月1日期间,106例患者入组并随机分配至VC-ESPB组(n = 53)和传统组(n = 53)。剔除5例患者后,共101例患者(VC-ESPB组,n = 50;传统组,n = 51)纳入分析。在术后48小时内,VC-ESPB组和对照组的累积AUC水平(静息时:160.08±38.00对164.94±31.00;差值[90% CI],-4.861[-16.308, 6.585])和累积AUC(活动时:209.64±28.98对212.59±33.11;差值[90% CI],-2.948[-13.236, 7.339])相似。静息和活动时累积AUC差值的90% CI上限未达到非劣效性界值(26.5)。在术后48小时内,VC-ESPB组和传统组的非甾体类抗炎药补救镇痛率相似(n = 16,32.0%对n = 11,21.6%;P = 0.236)。VC-ESPB组(n = 0,0%)和传统组(n = 0,0%)均未观察到与治疗相关的死亡。在VC-ESPB组,1例患者出现局部部位麻痹(n = 1,2.0%),另1例患者出现皮疹(n = 1,2.0%)。传统组1例患者术前出现皮疹(n = 1,2.0%)。VC-ESPB组术后恶心(n = 2,4.0%对n = 9,17.6%;P = 0.028)、呕吐(n = 1,2.0%对n = 8,15.7%;P = 0.031)发生率显著较低,主要并发症发生率也较低(n = 4,8.0%对n = 6,11.8%;P = 0.033)。
本研究表明,与传统阿片类药物术后疼痛管理方法相比,VC-ESPB在OMH术后疼痛管理中具有非劣效性,提示OMH术后实现无阿片类药物疼痛管理是可行的。
中国福建省科技联合创新基金;福建省卫生健康委员会青年科研项目;福建省医疗卫生中青年领军人才科研培养项目;中国福建省重点临床专科建设项目。