Zhang Jun, Jiang Peng, Gong Chunxia, Kong Wei, Tu Yuan, Huang Yuzhen, Liu Ying
Department of Gynecology, People's Hospital of Chongqing Banan District, Chongqing, China.
Department of Gynecology, The First Affiliated Hospital of Chongqing Medical University, Chongqing, China.
Front Oncol. 2023 Aug 28;13:1240786. doi: 10.3389/fonc.2023.1240786. eCollection 2023.
The aim of this study is to explore the consistency of P53 immunohistochemical expression between preoperative biopsy and final pathology in endometrial cancer (EC), and to predict the prognosis of patients based on the 4-tier P53 expression and classic clinicopathological parameters.
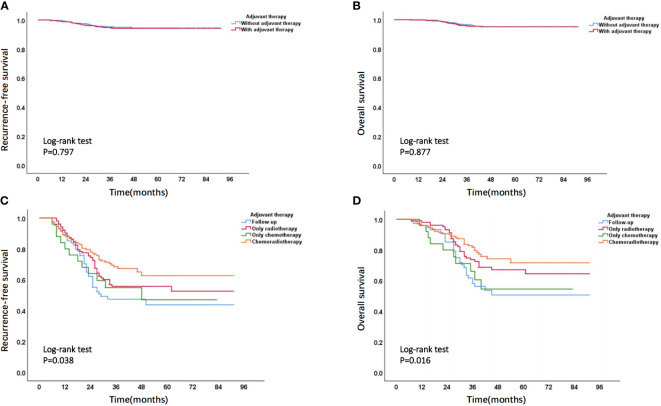
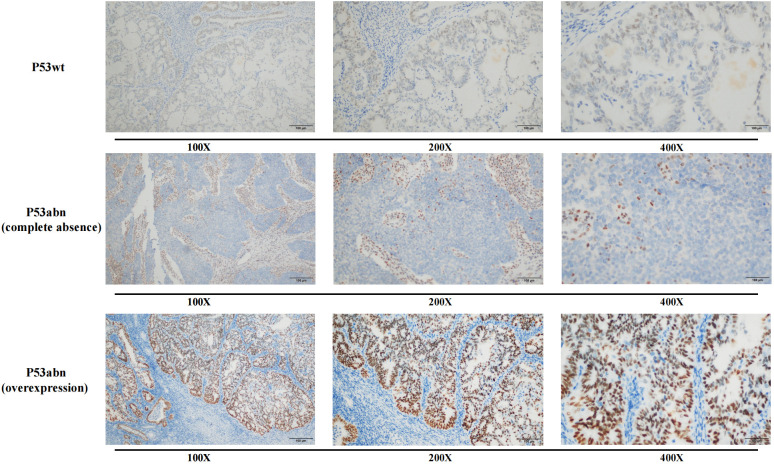
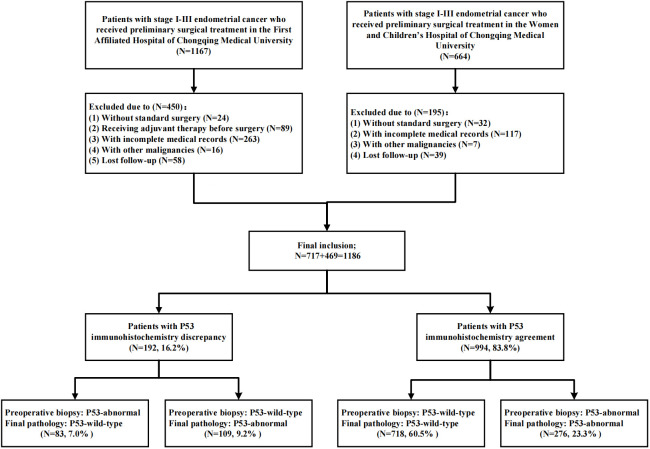
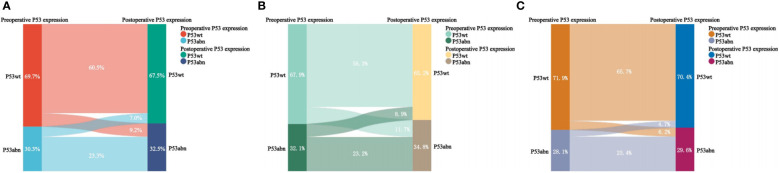
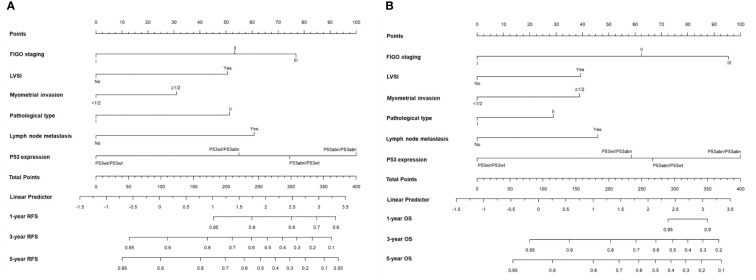
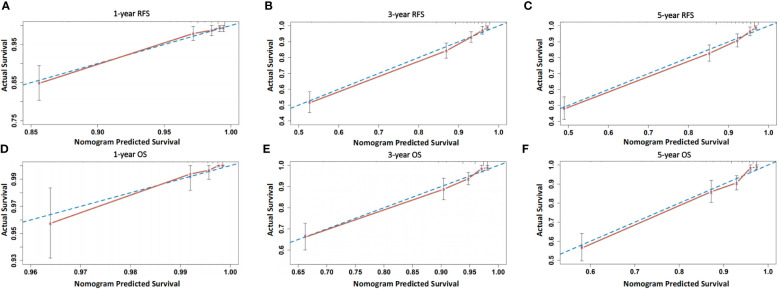
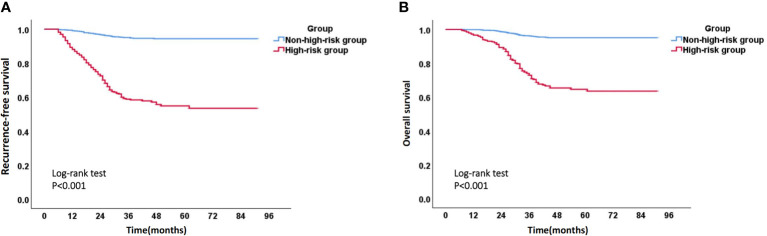
The medical data of patients with stage I-III EC who received preoperative biopsy and initial surgical treatment in two medical centers was retrospectively collected. The consistency of P53 immunohistochemistry expression between preoperative biopsy and final pathology was compared using Cohen's kappa coefficient and Sankey diagram, then 4-tier P53 expression was defined (P53wt/P53wt, P53abn/P53wt, P53wt/P53abn, and P53abn/P53abn). Univariate and multivariate Cox regression analysis was used to determine the correlation between 4-tier P53 expression and the prognosis of patients. On this basis, the nomogram models were established to predict the prognosis of patients by combining 4-layer P53 expression and classic clinicopathological parameters, then risk stratification was performed on patients.
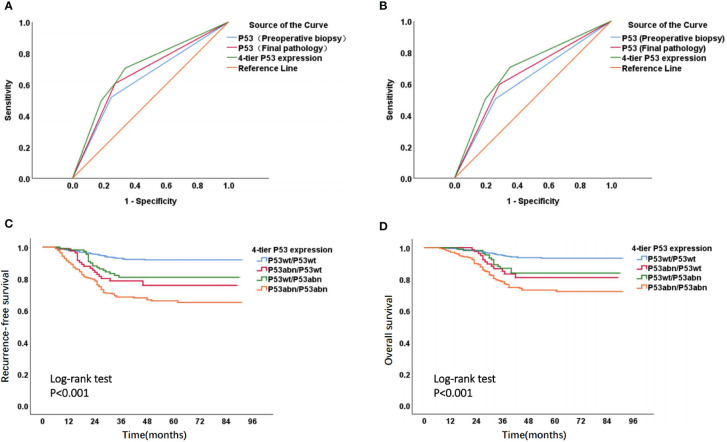
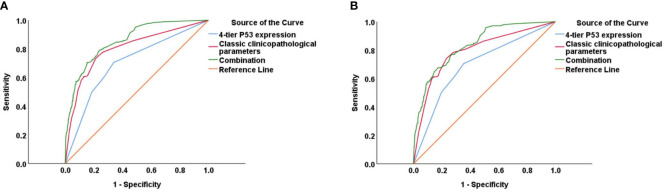
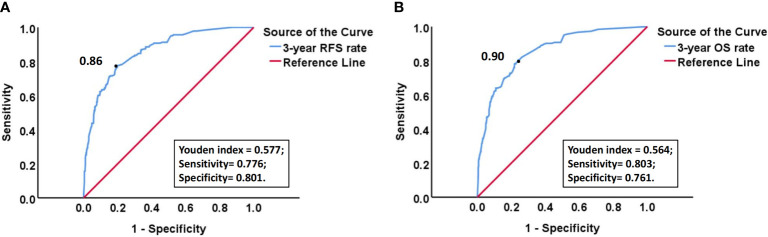
A total of 1186 patients were ultimately included in this study through inclusion and exclusion criteria. Overall, the consistency of P53 expression between preoperative biopsy and final pathology was 83.8%, with a kappa coefficient of 0.624. ROC curve suggested that the AUC of 4-tier P53 expression to predict the prognosis of patients was better than AUC of P53 expression in preoperative biopsy or final pathology alone. Univariate and multivariate Cox regression analysis suggested that 4-tier P53 expression was an independent influencing factor for recurrence and death. On this basis, the nomogram models based on 4-tier P53 expression and classical clinicopathological factors were successfully established. ROC curve suggested that the AUC (AUC for recurrence and death was 0.856 and 0.838, respectively) of the models was superior to the single 4-tier P53 expression or the single classical clinicopathological parameters, which could provide a better risk stratification for patients.
The expression of P53 immunohistochemistry had relatively good consistency between preoperative biopsy and final pathology of EC. Due to the discrepancy of P53 immunohistochemistry between preoperative biopsy and final pathology, the prognosis of patients can be better evaluated based on the 4-layer P53 expression and classic clinical pathological parameters.
本研究旨在探讨子宫内膜癌(EC)术前活检与最终病理中P53免疫组化表达的一致性,并基于4级P53表达和经典临床病理参数预测患者的预后。
回顾性收集在两个医疗中心接受术前活检和初始手术治疗的I-III期EC患者的医疗数据。使用Cohen's kappa系数和桑基图比较术前活检与最终病理中P53免疫组化表达的一致性,然后定义4级P53表达(P53wt/P53wt、P53abn/P53wt、P53wt/P53abn和P53abn/P53abn)。采用单因素和多因素Cox回归分析确定4级P53表达与患者预后的相关性。在此基础上,建立列线图模型,通过结合4层P53表达和经典临床病理参数预测患者预后,然后对患者进行风险分层。
通过纳入和排除标准,本研究最终共纳入1186例患者。总体而言,术前活检与最终病理中P53表达的一致性为83.8%,kappa系数为0.624。ROC曲线表明,4级P53表达预测患者预后的AUC优于单独术前活检或最终病理中P53表达的AUC。单因素和多因素Cox回归分析表明,4级P53表达是复发和死亡的独立影响因素。在此基础上,成功建立了基于4级P53表达和经典临床病理因素的列线图模型。ROC曲线表明,模型的AUC(复发和死亡的AUC分别为0.856和0.838)优于单一的4级P53表达或单一的经典临床病理参数,可为患者提供更好的风险分层。
EC术前活检与最终病理中P53免疫组化表达具有较好的一致性。由于术前活检与最终病理中P53免疫组化存在差异,基于4层P53表达和经典临床病理参数可更好地评估患者预后。