Huang Xin-Juan, Yin Man, Zhou Bing-Qian, Tan Xin-Yun, Xia Yuan-Qin, Qin Chun-Xiang
Xiangya Nursing of School, Central South University, Changsha 410013, Hunan Province, China.
School of Medicine, Jishou University, Jishou 416000, Hunan Province, China.
World J Hepatol. 2023 Aug 27;15(8):985-1000. doi: 10.4254/wjh.v15.i8.985.
Recently, a group of hepatologists proposed to rename non-alcoholic fatty liver disease (NAFLD) as metabolic associated fatty liver disease (MAFLD) with modified diagnostic criteria. It is important to note, however, that there are some differences between the diagnostic criteria used for NAFLD and MAFLD. Since the research on MAFLD is just beginning, however, evidence on its incidence and prevalence in the general population and in specific subpopulations remains limited.
To assess epidemiology of fatty liver in new definition and compare MAFLD with NAFLD. Exploring risk factors of MAFLD individuals.
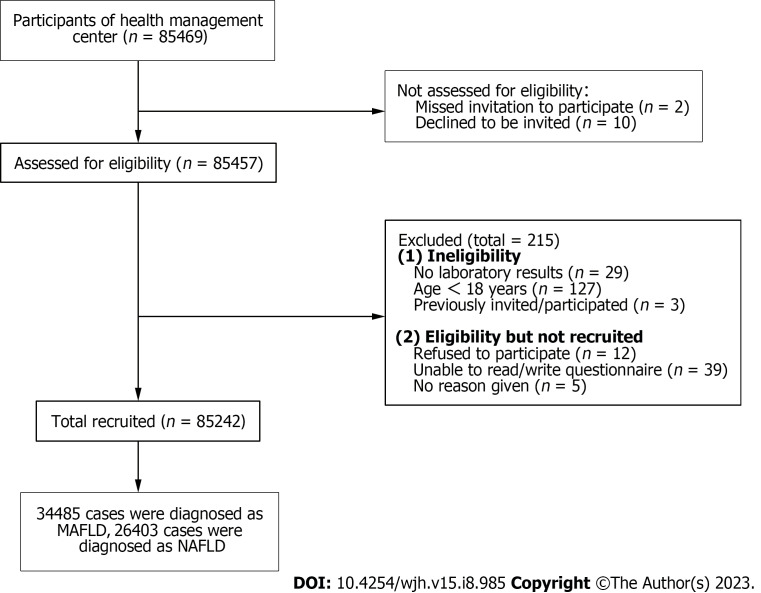
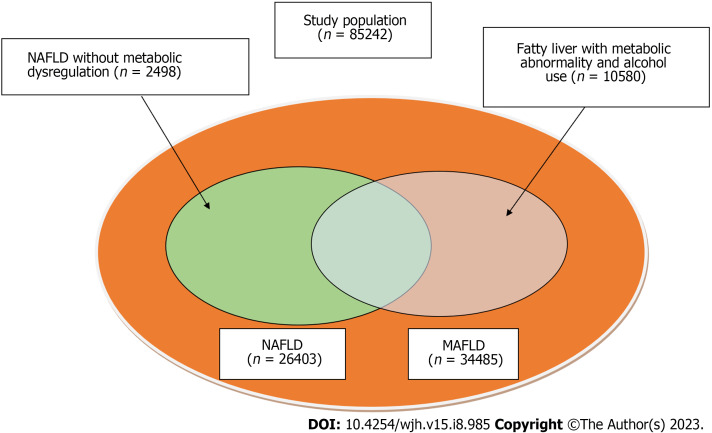
This was a retrospective, cross-sectional study. A total of 85242 adults were selected from the Chinese health management database in 2017-2022. The data of general information, laboratory indicators, lifestyle management and psychological status were obtained. MAFLD was diagnosed as ultrasound diagnosis of fatty liver and at least one between these three conditions: Overweight/obesity, type 2 diabetes mellitus (T2DM) or metabolic dysregulation. Metabolic factors were not considered in NAFLD diagnosis standard. The clinical characteristics of MAFLD and NAFLD were analysed using descriptive statistics. Continuous variables normally distributed were expressed as means ± SD. Categorical variables were expressed as frequencies and proportions. Binary logistic regression was used to determine risk factors of the MAFLD.
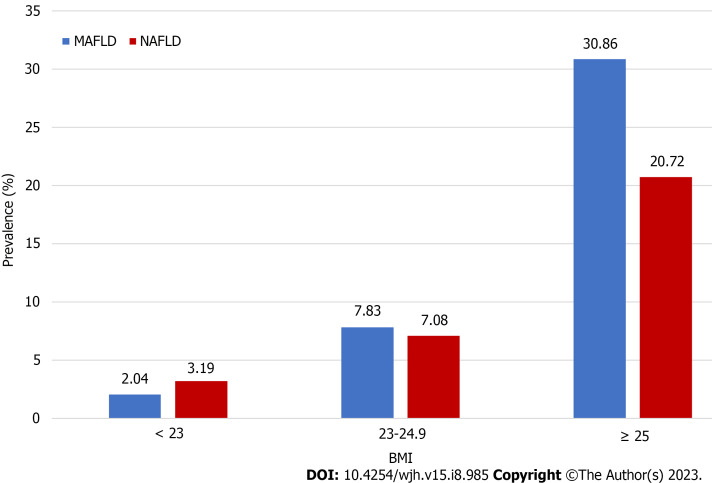
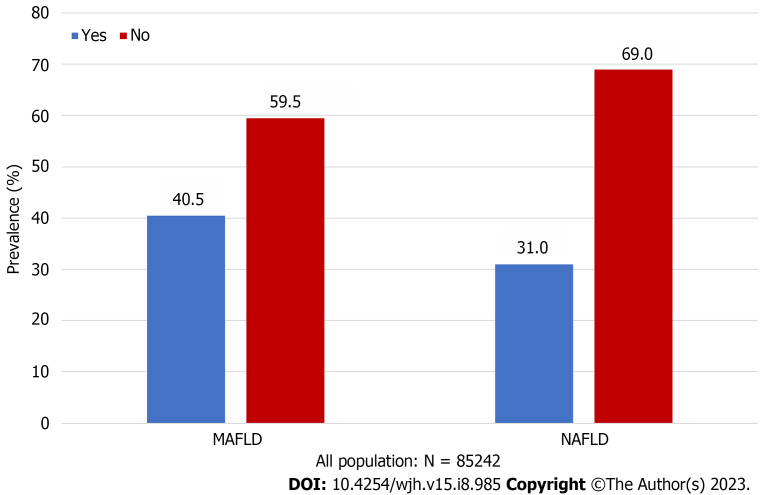
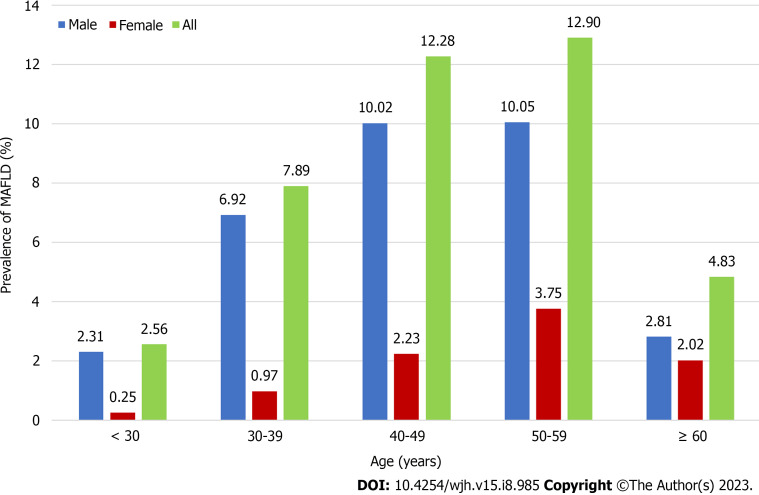
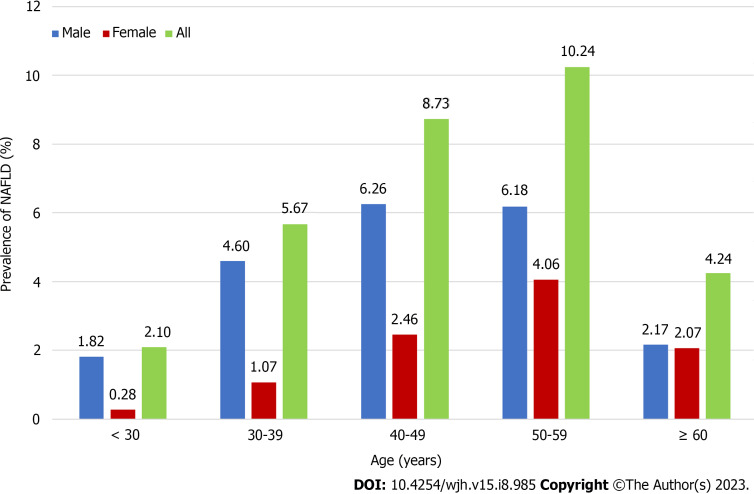
The prevalence of MAFLD and NAFLD was 40.5% and 31.0%, respectively. The MAFLD or NAFLD population is more likely to be older (M: 47.19 ± 10.82 43.43 ± 11.96; N: 47.72 ± 11.17 43.71 ± 11.66), male (M: 77.21% 44.43%; N: 67.90% 53.12%) and high body mass index (M: 26.79 ± 2.69 22.44 ± 2.48; N: 26.29 ± 2.84 23.29 ± 3.12) than the non-MAFLD or non-MAFLD population. In multivariate analysis, general information (, ≥ 2 metabolic abnormalities OR = 3.38, (95%CI: 2.99-3.81), < 0.001; diastolic blood pressure OR = 1.01, (95%CI: 1.00-1.01), = 0.002), laboratory results [,total bilirubin (TBIL) OR = 0.98, (95%CI: 0.98-0.99), < 0.001; serum uric acid(SUA) OR = 1.01, (95%CI: 1.01-1.01), < 0.001], and lifestyle factors [, drink beverage OR = 0.32, (95%CI: 0.17-0.63), = 0.001] were influence factors for MAFLD. Our study results offer new insight into potential risk factors associated with fatty liver disease, including SUA, TBIL and creatinine, all of which are related to chronic renal disease (CKD).
MAFLD is more prevalent than NAFLD, with two-fifths of individuals meeting the diagnosis criteria. MAFLD and NAFLD populations have different clinical characteristics. CKD may be related with MAFLD.
最近,一组肝病学家提议将非酒精性脂肪性肝病(NAFLD)重新命名为代谢相关脂肪性肝病(MAFLD),并修改了诊断标准。然而,需要注意的是,NAFLD和MAFLD的诊断标准存在一些差异。由于MAFLD的研究刚刚起步,其在普通人群和特定亚人群中的发病率和患病率的证据仍然有限。
评估新定义下脂肪肝的流行病学情况,并比较MAFLD和NAFLD。探索MAFLD个体的危险因素。
这是一项回顾性横断面研究。2017年至2022年从中国健康管理数据库中选取了85242名成年人。获取了一般信息、实验室指标、生活方式管理和心理状态的数据。MAFLD被诊断为超声诊断为脂肪肝,且符合以下三种情况中的至少一种:超重/肥胖、2型糖尿病(T2DM)或代谢失调。NAFLD诊断标准中未考虑代谢因素。采用描述性统计分析MAFLD和NAFLD的临床特征。正态分布的连续变量以均值±标准差表示。分类变量以频率和比例表示。采用二元逻辑回归确定MAFLD的危险因素。
MAFLD和NAFLD的患病率分别为40.5%和31.0%。MAFLD或NAFLD人群比非MAFLD或非NAFLD人群更可能年龄较大(男性:47.19±10.82对43.43±11.96;女性:47.72±11.17对43.71±11.66)、男性比例更高(男性:77.21%对44.43%;女性:67.90%对53.12%)且体重指数更高(男性:26.79±2.69对22.44±2.48;女性:26.29±2.84对23.29±3.12)。在多变量分析中,一般信息(≥2种代谢异常,OR = 3.38,95%CI:2.99 - 3.81,P < 0.001;舒张压,OR = 1.01,95%CI:1.00 - 1.01,P = 0.002)、实验室结果[总胆红素(TBIL),OR = 0.98,95%CI:0.98 - 0.99,P < 0.001;血清尿酸(SUA),OR = 1.01,95%CI:1.01 - 1.01,P < 0.001]和生活方式因素[饮用饮料,OR = 0.32,95%CI:0.17 - 0.63,P = 0.001]是MAFLD的影响因素。我们的研究结果为与脂肪性肝病相关的潜在危险因素提供了新的见解,包括SUA、TBIL和肌酐,所有这些都与慢性肾脏病(CKD)有关。
MAFLD比NAFLD更普遍,五分之二的个体符合诊断标准。MAFLD和NAFLD人群具有不同的临床特征。CKD可能与MAFLD有关。