Department of Radiology and Nuclear Medicine, Amsterdam UMC Location University of Amsterdam, Meibergdreef 9, 1105 AZ, Amsterdam, the Netherlands.
Department of Biomedical Engineering and Physics, Amsterdam UMC Location University of Amsterdam, Amsterdam, the Netherlands.
Eur Radiol. 2024 Apr;34(4):2152-2167. doi: 10.1007/s00330-023-10119-y. Epub 2023 Sep 20.
CT perfusion (CTP) has been suggested to increase the rate of large vessel occlusion (LVO) detection in patients suspected of acute ischemic stroke (AIS) if used in addition to a standard diagnostic imaging regime of CT angiography (CTA) and non-contrast CT (NCCT). The aim of this study was to estimate the costs and health effects of additional CTP for endovascular treatment (EVT)-eligible occlusion detection using model-based analyses.
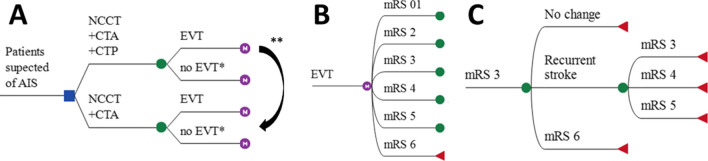
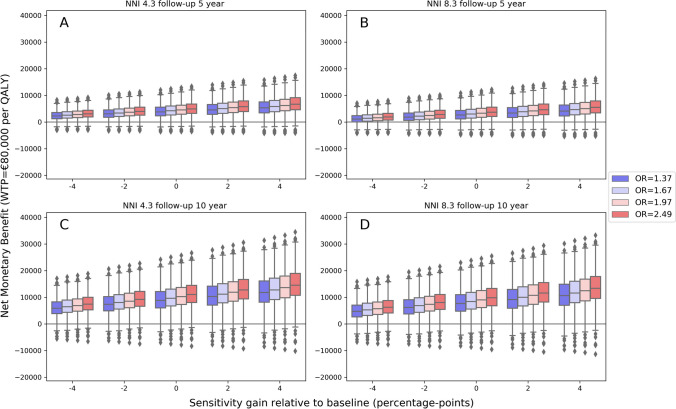
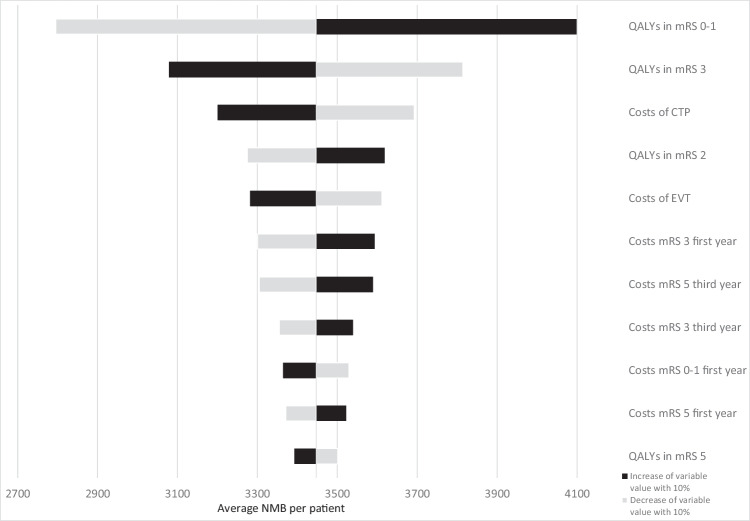
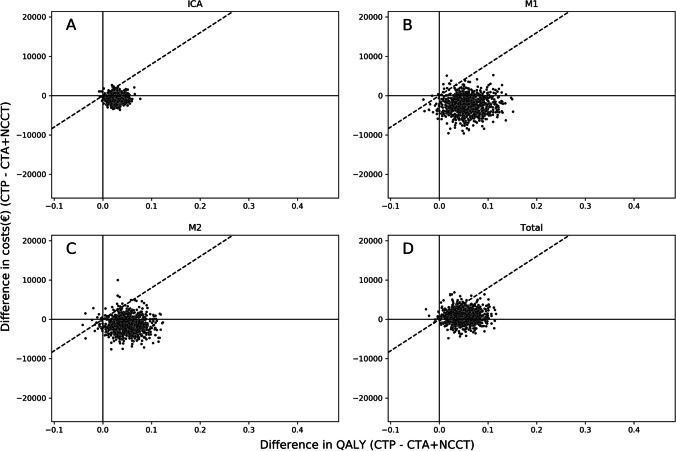
In this Dutch, nationwide retrospective cohort study with model-based health economic evaluation, data from 701 EVT-treated patients with available CTP results were included (January 2018-March 2022; trialregister.nl:NL7974). We compared a cohort undergoing NCCT, CTA, and CTP (NCCT + CTA + CTP) with a generated counterfactual where NCCT and CTA (NCCT + CTA) was used for LVO detection. The NCCT + CTA strategy was simulated using diagnostic accuracy values and EVT effects from the literature. A Markov model was used to simulate 10-year follow-up. We adopted a healthcare payer perspective for costs in euros and health gains in quality-adjusted life years (QALYs). The primary outcome was the net monetary benefit (NMB) at a willingness to pay of €80,000; secondary outcomes were the difference between LVO detection strategies in QALYs (ΔQALY) and costs (ΔCosts) per LVO patient.
We included 701 patients (median age: 72, IQR: [62-81]) years). Per LVO patient, CTP-based occlusion detection resulted in cost savings (ΔCosts median: € - 2671, IQR: [€ - 4721; € - 731]), a health gain (ΔQALY median: 0.073, IQR: [0.044; 0.104]), and a positive NMB (median: €8436, IQR: [5565; 11,876]) per LVO patient.
CTP-based screening of suspected stroke patients for an endovascular treatment eligible large vessel occlusion was cost-effective.
Although CTP-based patient selection for endovascular treatment has been recently suggested to result in worse patient outcomes after ischemic stroke, an alternative CTP-based screening for endovascular treatable occlusions is cost-effective.
• Using CT perfusion to detect an endovascular treatment-eligible occlusions resulted in a health gain and cost savings during 10 years of follow-up. • Depending on the screening costs related to the number of patients needed to image with CT perfusion, cost savings could be considerable (median: € - 3857, IQR: [€ - 5907; € - 1916] per patient). • As the gain in quality adjusted life years was most affected by the sensitivity of CT perfusion-based occlusion detection, additional studies for the diagnostic accuracy of CT perfusion for occlusion detection are required.
CT 灌注(CTP)已被建议在疑似急性缺血性卒中(AIS)患者中增加大血管闭塞(LVO)的检测率,如果与 CT 血管造影(CTA)和非对比 CT(NCCT)的标准诊断成像方案联合使用。本研究的目的是使用基于模型的分析来估计在血管内治疗(EVT)合格的闭塞检测中额外使用 CTP 的成本和健康效果。
这是一项来自荷兰的全国性回顾性队列研究,采用基于模型的健康经济学评估,纳入了 701 名接受 EVT 治疗且有 CTP 结果的患者(2018 年 1 月至 2022 年 3 月;trialregister.nl:NL7974)。我们比较了接受 NCCT、CTA 和 CTP(NCCT+CTA+CTP)的队列与假设 NCCT 和 CTA(NCCT+CTA)用于 LVO 检测的对照队列。NCCT+CTA 策略是使用文献中的诊断准确性值和 EVT 效果进行模拟的。使用马尔可夫模型模拟 10 年随访。我们从医疗保健支付者的角度考虑了欧元的成本和质量调整生命年(QALYs)的健康收益。主要结果是在支付意愿为 80000 欧元时的净货币收益(NMB);次要结果是 LVO 检测策略在 QALYs(ΔQALY)和成本(ΔCosts)方面的差异,每例 LVO 患者。
我们纳入了 701 名患者(中位年龄:72 岁,IQR:[62-81]岁)。与基于 CTP 的闭塞检测相比,每例 LVO 患者的成本节省(ΔCosts 中位数:-2671 欧元,IQR:[-4721 欧元;-731 欧元])、健康收益(ΔQALY 中位数:0.073,IQR:[0.044;0.104])和 NMB 为正(中位数:8436 欧元,IQR:[5565 欧元;11876 欧元])。
基于 CTP 的疑似卒中患者的血管内治疗合格大血管闭塞筛查具有成本效益。
尽管最近有研究表明,基于 CTP 的患者选择用于血管内治疗会导致缺血性卒中后患者预后恶化,但替代的基于 CTP 的血管内治疗可治疗的闭塞筛查具有成本效益。
使用 CT 灌注检测血管内治疗合格的闭塞可在 10 年随访期间带来健康获益和成本节省。
根据与需要 CT 灌注成像的患者数量相关的筛查成本,成本节省可能相当可观(中位数:-3857 欧元,IQR:[-5907 欧元;-1916 欧元])。
由于 CTP 基于闭塞检测的敏感性对质量调整生命年的增益影响最大,因此需要进行更多关于 CTP 对闭塞检测的诊断准确性的研究。