Academic Neurosurgery Unit, MCS Institute, St. George's, University of London, London, SW17 0RE, UK.
Neuroanaesthesia Department and Neuro Intensive Care Unit, St. George's Hospital, London, UK.
Neurocrit Care. 2021 Dec;35(3):794-805. doi: 10.1007/s12028-021-01232-1. Epub 2021 Jun 7.
Acute, severe traumatic spinal cord injury often causes fecal incontinence. Currently, there are no treatments to improve anal function after traumatic spinal cord injury. Our study aims to determine whether, after traumatic spinal cord injury, anal function can be improved by interventions in the neuro-intensive care unit to alter the spinal cord perfusion pressure at the injury site.
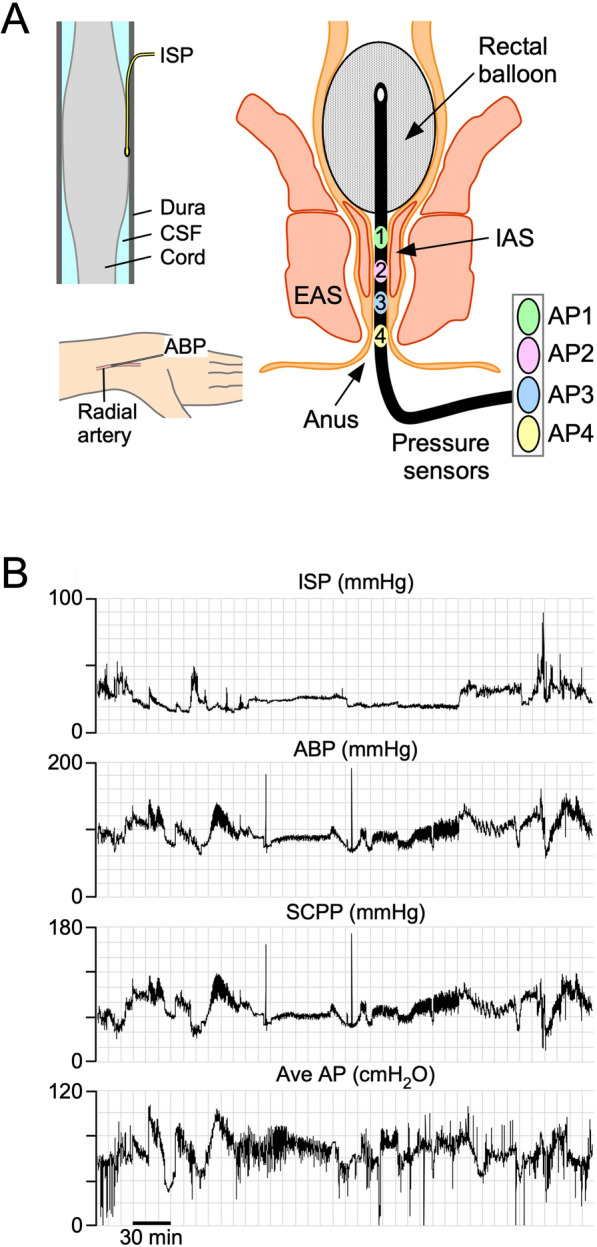
We recruited a cohort of patients with acute, severe traumatic spinal cord injuries (American Spinal Injury Association Impairment Scale grades A-C). They underwent surgical fixation within 72 h of the injury and insertion of an intrathecal pressure probe at the injury site to monitor intraspinal pressure and compute spinal cord perfusion pressure as mean arterial pressure minus intraspinal pressure. Injury-site monitoring was performed at the neuro-intensive care unit for up to a week after injury. During monitoring, anorectal manometry was also conducted over a range of spinal cord perfusion pressures.
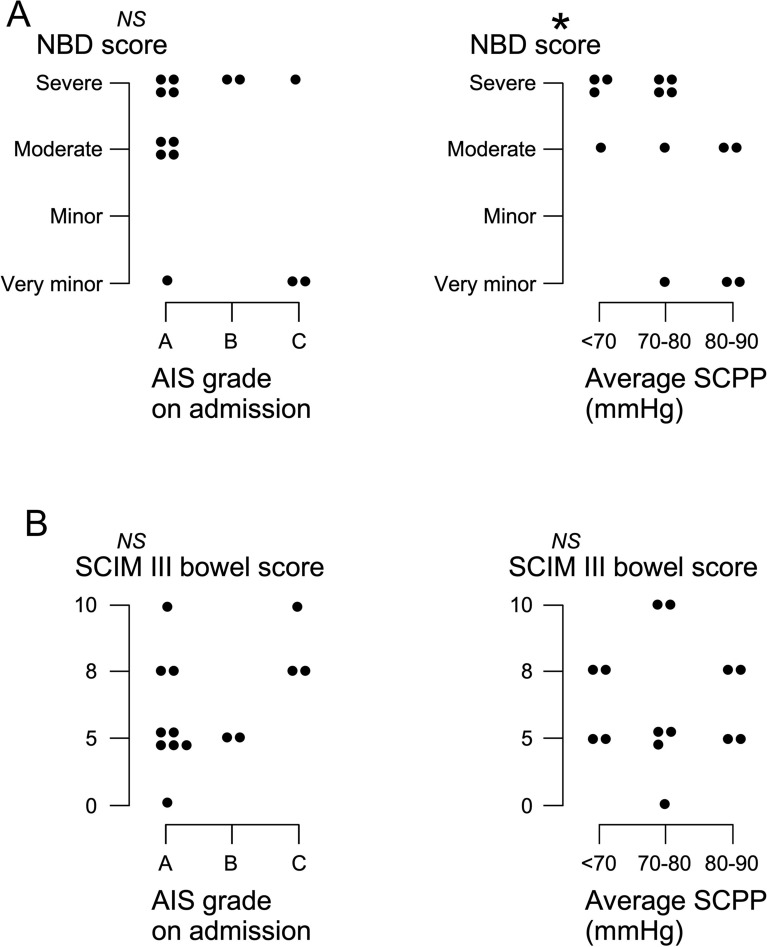
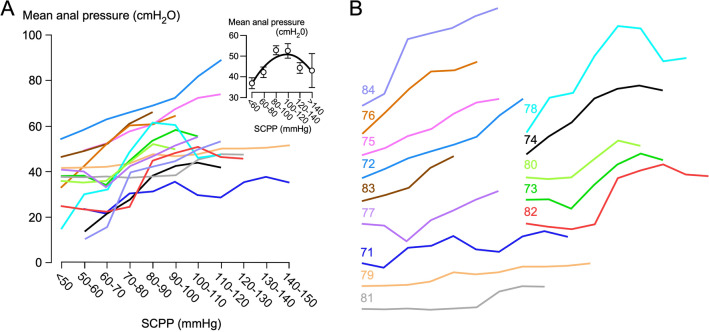
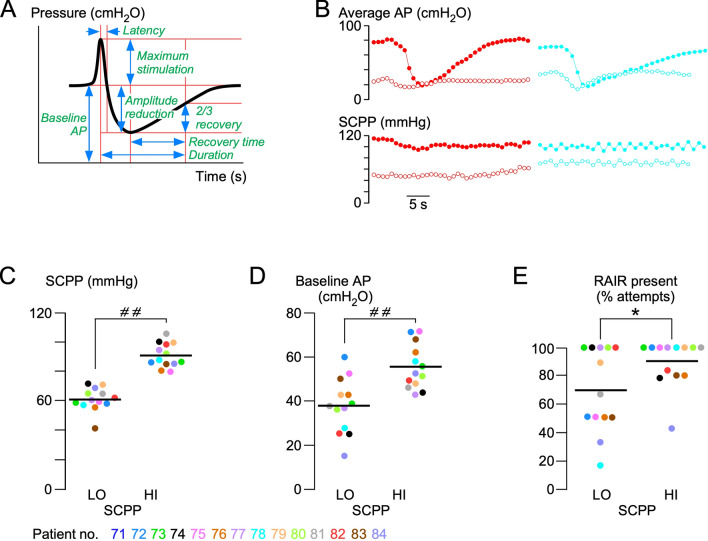
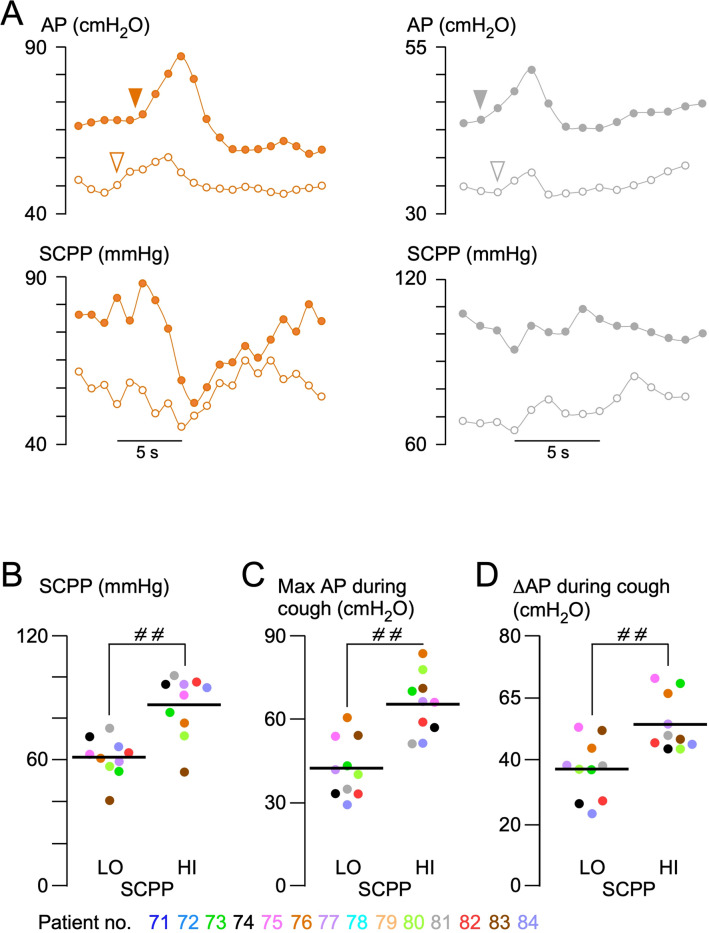
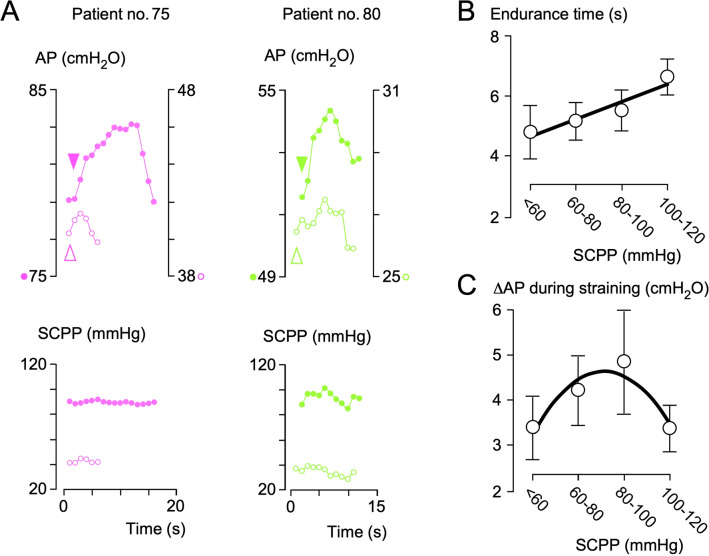
Data were collected from 14 patients with consecutive traumatic spinal cord injury aged 22-67 years. The mean resting anal pressure was 44 cmHO, which is considerably lower than the average for healthy patients, previously reported at 99 cmHO. Mean resting anal pressure versus spinal cord perfusion pressure had an inverted U-shaped relation (Ȓ = 0.82), with the highest resting anal pressures being at a spinal cord perfusion pressure of approximately 100 mmHg. The recto-anal inhibitory reflex (transient relaxation of the internal anal sphincter during rectal distension), which is important for maintaining fecal continence, was present in 90% of attempts at high (90 mmHg) spinal cord perfusion pressure versus 70% of attempts at low (60 mmHg) spinal cord perfusion pressure (P < 0.05). During cough, the rise in anal pressure from baseline was 51 cmHO at high (86 mmHg) spinal cord perfusion pressure versus 37 cmHO at low (62 mmHg) spinal cord perfusion pressure (P < 0.0001). During anal squeeze, higher spinal cord perfusion pressure was associated with longer endurance time and spinal cord perfusion pressure of 70-90 mmHg was associated with stronger squeeze. There were no complications associated with anorectal manometry.
Our data indicate that spinal cord injury causes severe disruption of anal sphincter function. Several key components of anal continence (resting anal pressure, recto-anal inhibitory reflex, and anal pressure during cough and squeeze) markedly improve at higher spinal cord perfusion pressure. Maintaining too high of spinal cord perfusion pressure may worsen anal continence.
急性、严重的创伤性脊髓损伤常导致大便失禁。目前,尚无治疗方法可改善创伤性脊髓损伤后的肛门功能。我们的研究旨在确定创伤性脊髓损伤后,通过改变损伤部位脊髓的灌注压,在神经重症监护病房进行干预是否可以改善肛门功能。
我们招募了一组急性、严重创伤性脊髓损伤(美国脊髓损伤协会损伤分级 A-C)的患者。他们在损伤后 72 小时内接受了手术固定,并在损伤部位插入了鞘内压力探头,以监测脊髓内压力并计算脊髓灌注压,即平均动脉压减去脊髓内压力。在损伤后一周内,在神经重症监护病房进行损伤部位监测。在监测过程中,还在一系列脊髓灌注压下进行了肛门直肠测压。
共收集了 14 例年龄在 22-67 岁的连续创伤性脊髓损伤患者的数据。静息肛门压力平均为 44cmHO,明显低于先前报道的健康患者的平均水平(99cmHO)。静息肛门压力与脊髓灌注压呈倒 U 形关系(Ȓ=0.82),最高的静息肛门压力出现在脊髓灌注压约为 100mmHg 时。直肠肛门抑制反射(直肠扩张时内肛门括约肌的短暂松弛)对维持粪便控制很重要,在 90mmHg 高脊髓灌注压下的尝试中有 90%存在,而在 60mmHg 低脊髓灌注压下的尝试中仅有 70%存在(P<0.05)。咳嗽时,静息肛门压力从基线上升 51cmHO,在 86mmHg 高脊髓灌注压下,而在 62mmHg 低脊髓灌注压下上升 37cmHO(P<0.0001)。在肛门挤压时,较高的脊髓灌注压与更长的耐力时间相关,70-90mmHg 的脊髓灌注压与更强的挤压相关。肛门直肠测压无并发症。
我们的数据表明,脊髓损伤导致肛门括约肌功能严重受损。肛门控便的几个关键组成部分(静息肛门压力、直肠肛门抑制反射和咳嗽及挤压时的肛门压力)在较高的脊髓灌注压下显著改善。维持过高的脊髓灌注压可能会使肛门控便恶化。