Zhang Baihua, Guo Xiaotong, Jia Ran, Wang Zhan, Wu Jie, Chen Xiaoyan, Li Jigang, Yang Desong, Li Xu, Wang Wenxiang, Xiao Qin
Department of Thoracic Surgery, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital and Shenzhen Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Shenzhen, China.
Department of Thoracic Surgery, Hunan Clinical Medical Research Center of Accurate Diagnosis and Treatment for Esophageal Carcinoma, Hunan Cancer Hospital and The Affiliated Cancer Hospital of Xiangya School of Medicine, Central South University, Changsha, Hunan, China.
Front Oncol. 2023 Sep 5;13:1200625. doi: 10.3389/fonc.2023.1200625. eCollection 2023.
Neoadjuvant chemoimmunotherapy is the optimal choice in the treatment of NSCLC; however, the optimal number of therapeutic cycles remains unclear. The primary aim of this study was to determine the optimal number of neoadjuvant therapeutic cycles in NSCLC.
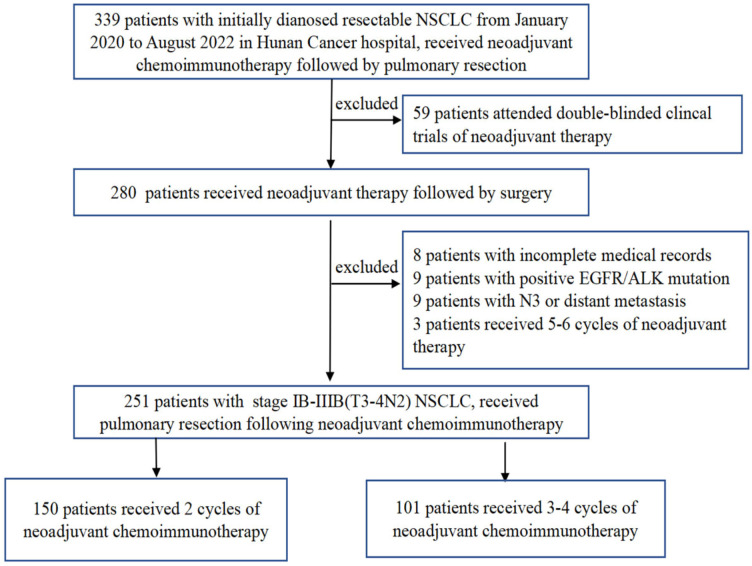
This study was a real-world clinical analysis that included patients who received neoadjuvant chemoimmunotherapy followed by surgery from January 2020 to August 2022. Patients were divided into two groups based on the number of therapeutic cycles: 2-cycle group and 3-4-cycles group. The primary endpoint was the major pathological response (MPR) rate.
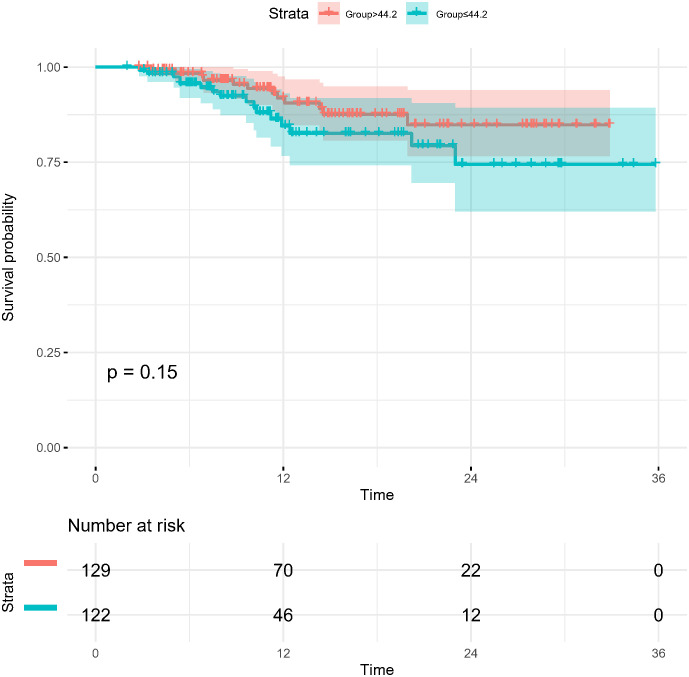
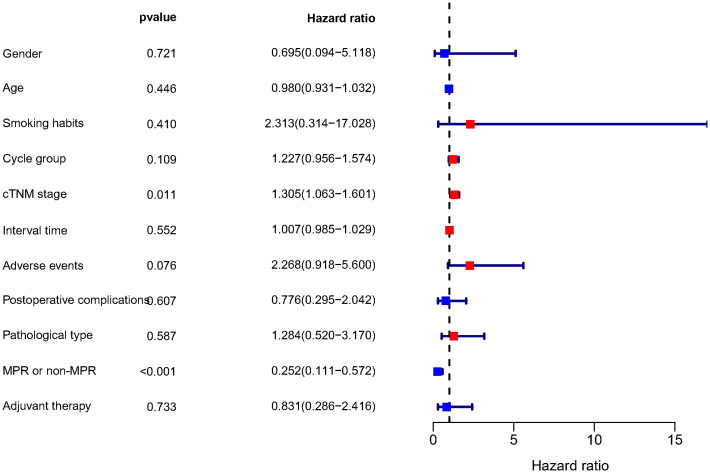
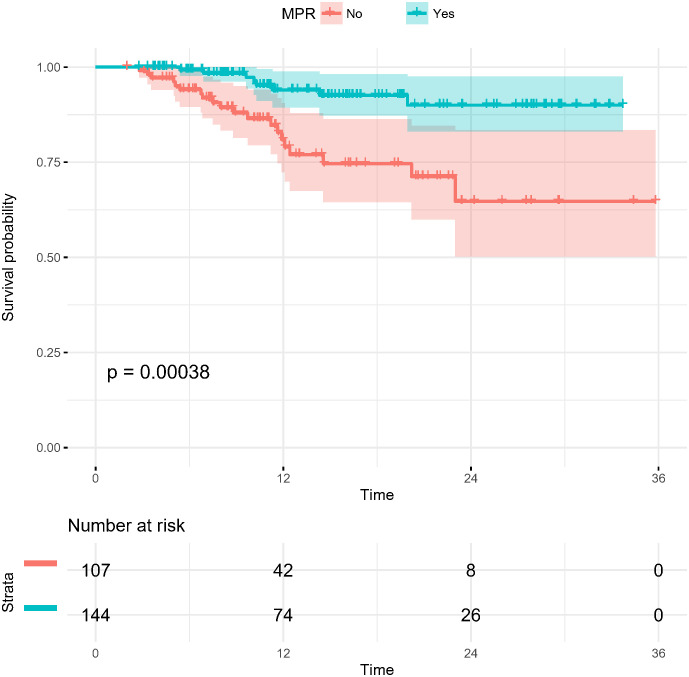
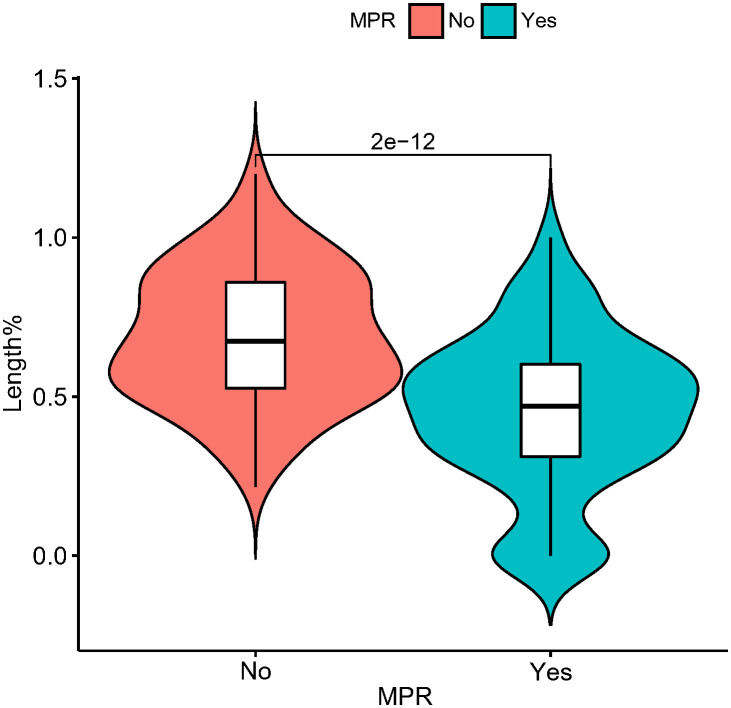
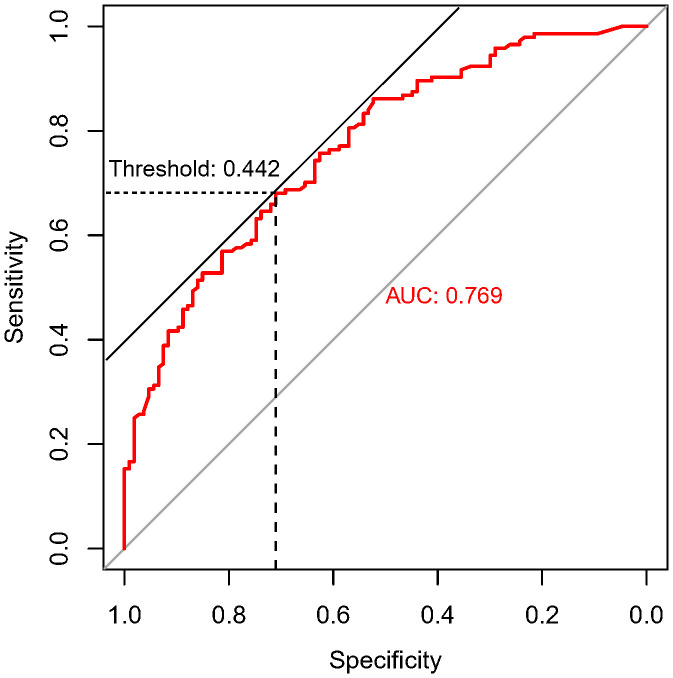
A total of 251 patients were included: 150 in the 2-cycle group and 101 in the 3-4-cycles group. Baseline characteristics were well-balanced between the groups. The MPR in the 2-cycle group was 57.3% and not significantly different from that of 57.4% in the 3-4-cycles group (p=0.529). Thirty-two patients (31.7%) in the 3-4-cycles group underwent surgery > 42 days after the final cycle of neoadjuvant therapy, significantly more than the 24 patients (16.0%) in the 2-cycle group (p=0.003). The incidence of adverse events related to neoadjuvant therapy was higher in the 3-4-cycles vs 2-cycle groups (72.3% versus 58.0%, respectively; p=0.021), while the 2-cycle group had a higher rate of postoperative morbidities (28.0% versus 12.9%, respectively; p=0.004). Additionally, for patients with ≤ 44.2% regression in diameter on computed tomography after two cycles of treatment, the MPR rate was higher in the 3-4-cycles vs 2-cycle group (47.3% versus 29.9%, respectively; p=0.048). For cases with programmed death-ligand 1 expression, regarding tumor proportion score ≤ 10%, 3-4 cycles of neoadjuvant treatment increased the MPR rate compared with 2 cycles (37.5% versus 9.5%, respectively; p=0.041).
Our data support the positive role of chemoimmunotherapy in the neoadjuvant treatment of NSCLC. Extending to 3-4 cycles instead of 2 cycles of neoadjuvant chemoimmunotherapy may improve the safety of surgery and result in a lower incidence of postoperative morbidities; however, the MPR rate may not increase significantly. CT re-evaluation during treatment and PD-L1 expression at initial diagnosis are potential indicators to guide the choice of the number of therapeutic cycles.
新辅助化疗免疫疗法是治疗非小细胞肺癌(NSCLC)的最佳选择;然而,最佳治疗周期数仍不明确。本研究的主要目的是确定NSCLC新辅助治疗的最佳周期数。
本研究是一项真实世界临床分析,纳入了2020年1月至2022年8月接受新辅助化疗免疫治疗后行手术的患者。根据治疗周期数将患者分为两组:2周期组和3 - 4周期组。主要终点是主要病理缓解(MPR)率。
共纳入251例患者:2周期组150例,3 - 4周期组101例。两组间基线特征均衡。2周期组的MPR为57.3%,与3 - 4周期组的57.4%无显著差异(p = 0.529)。3 - 4周期组有32例患者(31.7%)在新辅助治疗最后一个周期后> 42天接受手术,显著多于2周期组的24例患者(16.0%)(p = 0.003)。新辅助治疗相关不良事件的发生率在3 - 4周期组高于2周期组(分别为72.3%和58.0%;p = 0.021),而2周期组术后并发症发生率更高(分别为28.0%和12.9%;p = 0.004)。此外,对于治疗两个周期后计算机断层扫描直径缩小≤ 44.2%的患者,3 - 4周期组的MPR率高于2周期组(分别为47.3%和29.9%;p = 0.048)。对于程序性死亡配体1表达的病例,肿瘤比例评分≤ 10%时,与2周期新辅助治疗相比,3 - 4周期新辅助治疗可提高MPR率(分别为37.5%和9.5%;p = 0.041)。
我们的数据支持化疗免疫疗法在NSCLC新辅助治疗中的积极作用。将新辅助化疗免疫疗法延长至3 - 4周期而非2周期可能会提高手术安全性并降低术后并发症发生率;然而,MPR率可能不会显著提高。治疗期间的CT重新评估和初始诊断时的PD - L1表达是指导治疗周期数选择的潜在指标。