Department of Obstetrics, Ghent University Hospital, Vrouwenkliniek, Corneel Heymanslaan 10, 9000, Ghent, Belgium.
Department of Gynaecology and Obstetrics, Université Libre de Bruxelles (ULB) Hôpital Universitaire de Bruxelles (H.U.B.), Hôpital Erasme, Route de Lennik 808, Brussels, 1070, Belgium.
BMC Pregnancy Childbirth. 2023 Sep 22;23(1):684. doi: 10.1186/s12884-023-05984-w.
Trial of Labor After Cesarean is an important strategy for reducing the overall rate of cesarean delivery. Offering the option of vaginal delivery to a woman with a history of cesarean section requires the ability to manage a potential uterine rupture quickly and effectively. This requires infrastructure and organization of the maternity unit so that the decision-to-delivery interval is as short as possible when uterine rupture is suspected. We hypothesize that the organizational characteristics of maternity units in Belgium have an impact on their proposal and success rates of trial of labour after cesarean section.
We collected data on the organizational characteristics of Belgian maternity units using an online questionnaire. Data on the frequency of cesarean section, trial of labor and vaginal birth after cesarean section were obtained from regional perinatal registries. We analyzed the determinants of the proposal and success of trial of labor after cesarean section and report the associations as mean proportions.
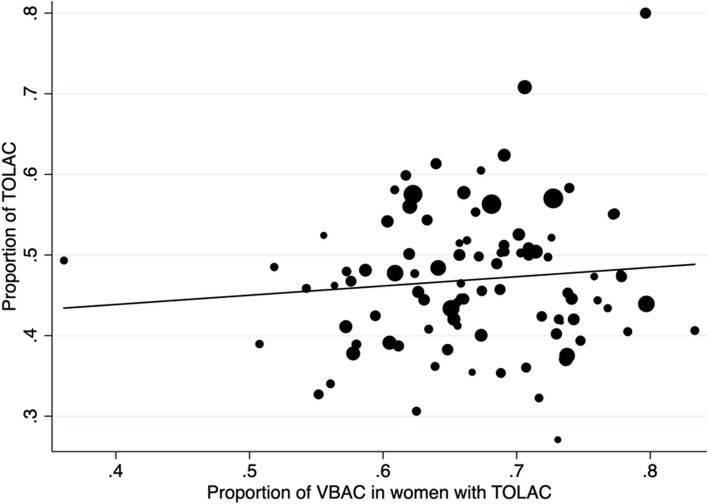
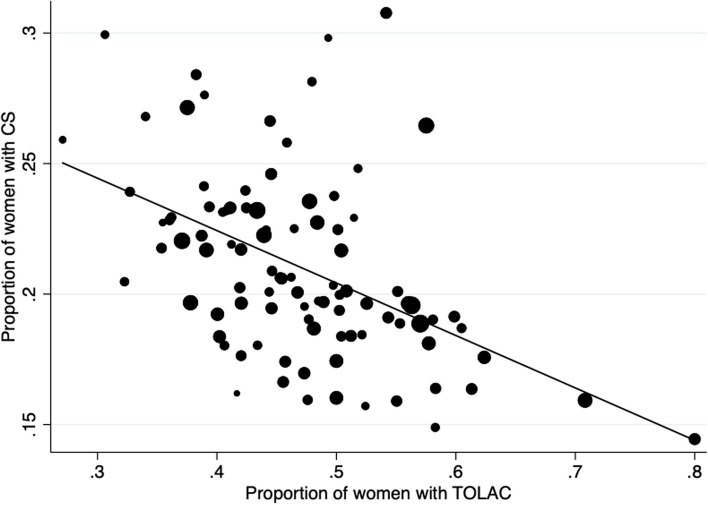
Of the 101 maternity units contacted, 97 responded to the questionnaire and data from 95 was included in the analysis. Continuous on-site presence of a gynecologist and an anesthetist was associated with a higher proportion of trial of labor after cesarean section, compared to units where staff was on-call from home (51% versus 46%, p = 0.04). There is a non-significant trend towards more trial of labor after cesarean section in units with an operating room in or near the delivery unit and a shorter transfer time, in larger units (> 1500 deliveries/year) and in units with a neonatal intensive care unit. The proposal of trial of labor after cesarean section and its success was negatively correlated to the number of cesarean section in the maternity unit (Spearman' rho = 0.50 and 0.42, p value < 0.001).
Organizational differences in maternity units appear to affect the proposal of trial of labor after cesarean section. Addressing these organizational factors may not be sufficient to change practice, given that general tendency to perform a cesarean section in the maternity unit is the main contributor to the percentage of trial of labor after cesarean.
剖宫产术后试产是降低剖宫产率的重要策略。为有剖宫产史的妇女提供阴道分娩的选择,需要能够快速有效地处理潜在的子宫破裂。这需要产科单位的基础设施和组织,以便在怀疑子宫破裂时将决策与分娩的间隔时间尽可能缩短。我们假设比利时产科单位的组织特征对其剖宫产术后试产的建议和成功率有影响。
我们使用在线问卷收集了比利时产科单位的组织特征数据。从区域围产期登记处获得剖宫产、试产和剖宫产后阴道分娩的频率数据。我们分析了剖宫产术后试产建议和成功的决定因素,并报告了关联的平均比例。
在联系的 101 家产科单位中,有 97 家对问卷做出了回应,其中 95 家的数据纳入了分析。与从家中值班的单位相比,连续在场的妇科医生和麻醉师与更高的剖宫产术后试产比例相关(51%对 46%,p=0.04)。在手术室位于或靠近产房且转移时间较短的单位、规模较大的单位(>1500 例分娩/年)和有新生儿重症监护病房的单位中,剖宫产术后试产的比例呈上升趋势,但无统计学意义。剖宫产术后试产的建议及其成功率与产科单位的剖宫产数量呈负相关(Spearman rho分别为 0.50 和 0.42,p 值均<0.001)。
产科单位的组织差异似乎影响了剖宫产术后试产的建议。考虑到产科单位进行剖宫产的总体趋势是影响剖宫产后试产比例的主要因素,解决这些组织因素可能不足以改变实践。